0254
Intermuscular Variability of Phosphocreatine Recovery Constants in Exercised Muscle Measured using 31PMRS and CrCEST at 7.0T1Radiology, University of Pennsylvania, Philadelphia, PA, United States, 2Siemens Medical Solutions USA Inc, Malvern, PA, United States
Synopsis
Synopsis: As a noninvasive imaging biomarker, phosphorous magnetic resonance spectroscopy (31PMRS) has traditionally been used to measure the metabolic response of exercised skeletal muscle in humans and has contributed immensely to the vital understanding of muscle energetics. However, due to lack of spatial resolution in 31PMRS, it is difficult to resolve the intermuscular variabilities of creatine kinase kinetics. In this study we demonstrate that with proper placement of surface coil in a mild exercise study, the recovery constant for PCr determined from 31PMRS matches well with recovery constant measured from CrCEST using a volume coil for the same muscle group.
Introduction
Systemic energy deficiency, traditionally measured as the delayed phosphocreatine (PCr) recovery, has been the part of pathophysiology in various disorders, such as primary mitochondrial disorders(1), muscle injury(2), cardiovascular disease(3) and diabetes mellitus(4). Under mild exercise regimens, creatine weighted chemical exchange saturation transfer or CrCEST(5) has proven its potential to detect abnormal CK kinetics in mitochondrial diseases(3). 31PMRS can be used both in mild and severe exercise regimens and can provide information on the other species of CK kinetics, such as inorganic phosphate, acidity, ATP (adenosine triphosphate). In our previous studies(5), the recovery time constant for PCr derived from 31PMRS was shorter by >20-30% than the recovery time constant derived from CrCEST. Here, we demonstrate that with proper surface coil placement depending upon the geometry of the individual calf muscle groups, one can detect inter-muscular variability using 31PMRS localized using surface coil placement and the recovery constants derived from 31PMRS and CrCEST are within 10% for different muscle groups.Methods
All plantar flexion exercise (PFE) studies were conducted using a MR compatible pneumatical ergometer (Trispect, Ergospect, Innsbruck, Austria) was used in the manual mode. The applied air pressure was kept at 8 psi (pound per square inch) and the pedaling frequency was kept at 30 beats per minute (BPM). The IRB approved human studies were conducted on 7T MRI scanner (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany).31PMRS: 31PMRS data were acquired on two volunteers using a commercial 7 cm diameter dual tuned 31P-1H transmit/receive surface coil (O-XL-HL-070-01379-001 V01; RAPID Biomedical GMBH, Rimpar, Germany) mounted on a custom built stand. Different volumes of calf muscles were excited using three different placements of surface coil, as shown in Fig, 1. Lateral gastrocnemius (LG) and medial gastrocnemius (MG) were the single major contributors for two “extreme” placements of coil, whereas mixed contributions from LG, MG were observed when the coil was placed right beneath the calf muscle. 31PMRS data from two volunteers were acquired using different coil positions in the same session. For reproducibility testing, for one volunteer, three repetitions were performed on these different days within a week. Between different PFEs, a gap of approximately 20 minutes was maintained to allow for the full PCr recovery.
CrCEST: CrCEST MRI studies were performed using a commercial 28Channel Knee coil (Quality Electrodynamics, USA). The prototype sequence consisted of the pulse train (5x100ms Hanning-windowed, duty-cycle 99%, B1rms =2.9μT), followed by single shot GRE read out with TR= 3.5ms, TE =1.47ms, BW=710Hz/pixel, with a T1 recovery delay of 5 seconds. Other imaging parameters were: Voxel size 1.4x1.4x5mm3; FOV =160x160; FOV phase 100%; averaging 1; # slices =8; BW =710Hz; Turbo factor =422. Spiral with elliptical scanning in transverse orientation. CEST imaging was accelerated using GRAPPA with acceleration factors: along PE=2, along 3D=1, Reference lines =24. Raw CEST images were acquired at six saturation offset frequencies from ±1.5, ±1.8, ±2.1ppm (relative to water resonance set as 0ppm). WASSR images (from ±0 to ±0.9 ppm with a step-size of ±0.15 ppm), with a saturation pulse at B1rms of 0.29μT with 200ms duration, was used to correct for B0 in homogeneities(6). For B1-correction, linear correction was used.
Results
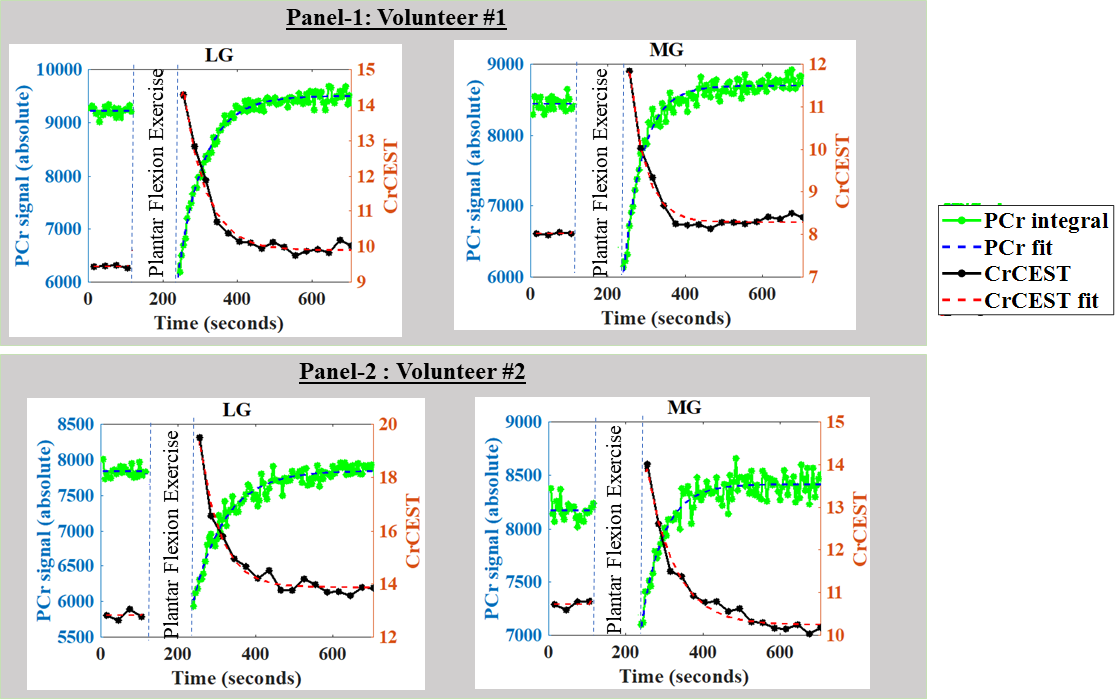
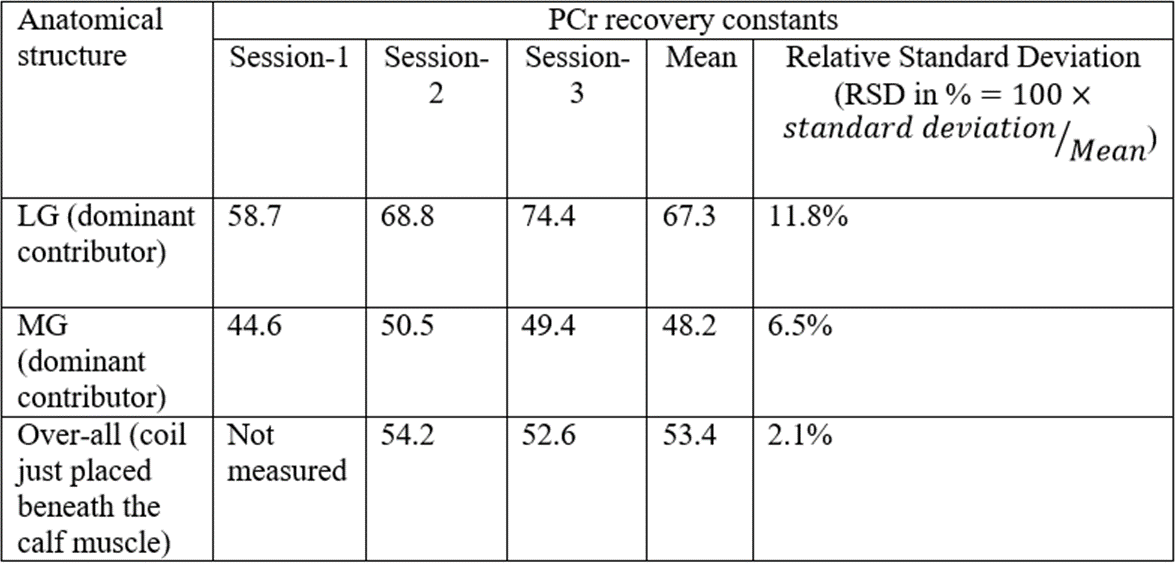
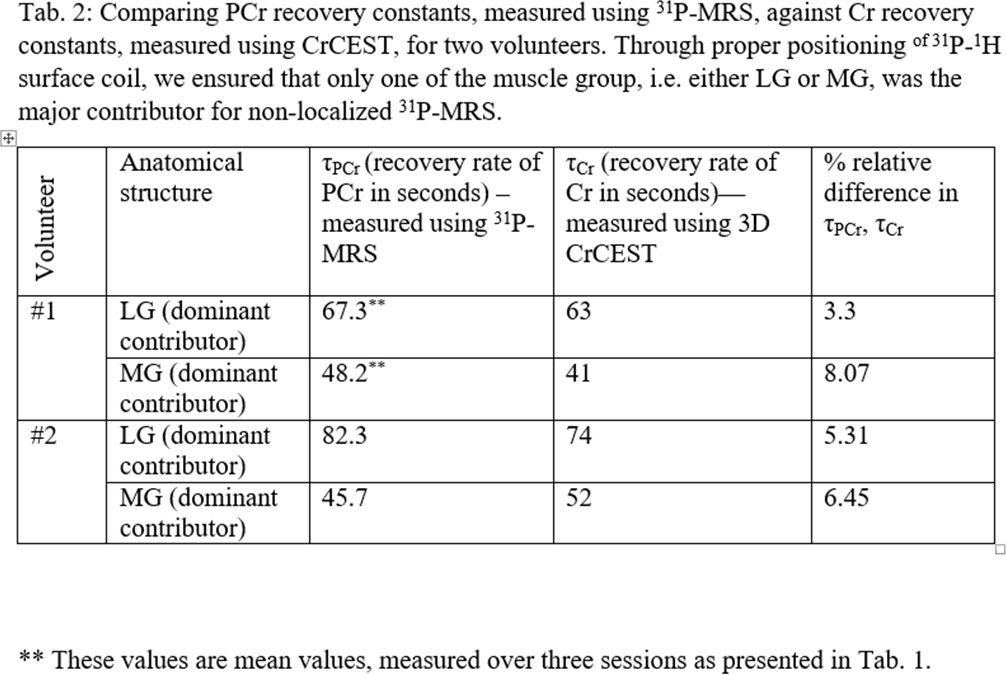
Results: With no shift in Pi peak, 31PMRS confirmed that that there was no pH change during mild PFE for given exercise workload. As expected, the Pi peak was found to be elevated immediately post exercise, which returned back to normal post exercise. PCr recovery measurements for volunteer #1 was repeated in three different sessions. As shown in Tab. 1, these repeated measurements demonstrated the presence of inter-muscular variability with respect to PCr recovery kinetics, with the mean values of Cr recovery time constant in LG and MG to be in 67.3, 48.2s respectively. The mean Cr recovery constant for the case when the coil was directly placed beneath the calf muscle was 53.4s. The relative standard deviation (RSD) of the PCr recovery rate, defined as the standard deviation normalized by the mean of the experiment, was highest (11.82%) for the case when LG was the main contributor and lowest (2.11%) for the case when the coil were placed right beneath the calf muscle. Additionally, PCr recovery curves of volunteer 2 was also measured for only two different placements of coils where LG and MG were single major contributors and the presence of inter-muscular variability with respect to PCr recovery kinetics were again very noticeable (Tab. 2). For both volunteers (#1,#2), PCr recovery rates measured using 31PMRS matched quite well (Fig. 2) with respective Cr recovery rate measured using CrCEST with relative difference between 3.3-8.07% (Tab. 2).Discussion
The rate constant of Cr/PCr recovery depends on numerous factors, including the intensity of exercise and work load, exercise conditions (aerobic/anaerobic), ergometer design, as well as biological/physiological variations in addition to methodological variations with origins in acquisition and processing. Under mild exercise conditions, the recovery rate constants derived from CrCEST MRI and 31PMRS are comparable for the same muscle groups.Conclusions
We demonstrated the presence of intermuscular variabilities both in CrCEST MRI and 31PMRS based PCr recovery. We found <10% difference between recovery time constants derived from 31PMRS and CrCEST for different muscle groups.Acknowledgements
This project was supported by National Institute of Biomedical Imaging and Bioengineering of the National Institute of Health through grant number P41-EB015893 (NIH/NIBIB) and R56-AG062665 (NIH).References
DeBrosse C, Nanga RPR, Wilson N, D'Aquilla K, Elliott M, Hariharan H, Yan F, Wade K, Nguyen S, Worsley D, Parris-Skeete C, McCormick E, Xiao R, Cunningham ZZ, Fishbein L, Nathanson KL, Lynch DR, Stallings VA, Yudkoff M, Falk MJ, Reddy R, McCormack SE. Muscle oxidative phosphorylation quantitation using creatine chemical exchange saturation transfer (CrCEST) MRI in mitochondrial disorders. JCI Insight 2016;1(18):e88207.
2. Armstrong RB, Warren GL, Warren JA. Mechanisms of exercise-induced muscle fibre injury. Sports Med 1991;12(3):184-207.
3. Ooi DS, Isotalo PA, Veinot JP. Correlation of antemortem serum creatine kinase, creatine kinase-MB, troponin I, and troponin T with cardiac pathology. Clin Chem 2000;46(3):338-344.
4. Popovich BK, Boheler KR, Dillmann WH. Diabetes decreases creatine kinase enzyme activity and mRNA level in the rat heart. Am J Physiol 1989;257(4 Pt 1):E573-577.
5. Kogan F, Haris M, Singh A, Cai K, Debrosse C, Nanga RP, Hariharan H, Reddy R. Method for high-resolution imaging of creatine in vivo using chemical exchange saturation transfer. Magn Reson Med 2014;71(1):164-172.
6. Kim M, Gillen J, Landman BA, Zhou J, van Zijl PC. Water saturation shift referencing (WASSR) for chemical exchange saturation transfer (CEST) experiments. Magn Reson Med 2009;61(6):1441-1450.
7. Kogan F, Haris M, Debrosse C, Singh A, Nanga RP, Cai K, Hariharan H, Reddy R. In vivo chemical exchange saturation transfer imaging of creatine (CrCEST) in skeletal muscle at 3T. J Magn Reson Imaging 2014;40(3):596-602.
Figures
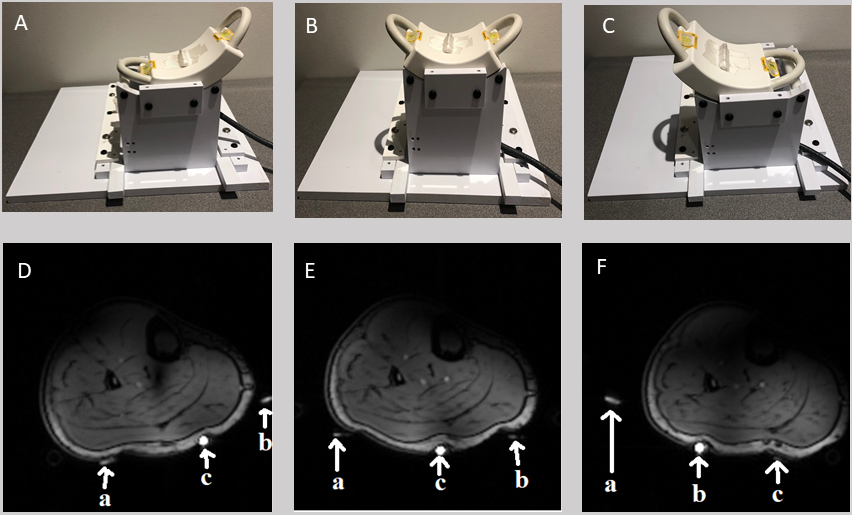
Fig. 1: Three different placements of 31P-1H surface coil (A,B,C) and respective localizer images (D, E, F) showing the positions calf muscle with respect to fiducial markers (marked by ‘a’, ‘b’) and a small vial containing PBS solution (marked by ‘c’). Whereas fiducial markers are indicating two ends of the coil, the location of vial roughly indicates middle portion of the coil.
An earlier study (7) using the same coil showed that the majority of the FID signal (85%) from the surface coil is obtained from a depth less than 1.8 cm from the coil.