0114
No substantial peripheral nerve stimulation beyond 5000T/m/s when driving a head gradient coil at 20kHz1Donders Institute for Brain, Cognition and Behavior, Radboud University Nijmegen, Nijmegen, Netherlands, 2Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 3Erwin L. Hahn Institute for Magnetic Resonance Imaging, University of Duisburg-Essen, Essen, Germany, 4Spinoza Center for Neuroimaging Amsterdam, Amsterdam, Netherlands
Synopsis
In this work the PNS threshold of a recently introduced gradient head coil operating at 20kHz was determined in four healthy subjects. The gradient slew rate was increased to 5000T/m/s by varying the amplitude between 7.5–40mT/m, the maximal gradient strength currently available. One subject reported no PNS, two subjects reported mild PNS at the highest gradient amplitudes of 36.25, 37.5 and 40mT/m, and one subject reported mild sensations during 31.25mT/m, but was uncertain whether this was PNS. In conclusion, application of the coil at 20kHz is currently restricted by the available gradient strength, rather than PNS.
Background
Recently a silent z-axis gradient insert head coil that operates at 20kHz was introduced 1. The use of this high frequency brings the advantage of scanning outside the human hearing perception frequency ranges, thus making the gradient insert silent. Moreover, it can enhance the slew rate 25-fold (from 200T/m/s with body gradients to over 5000T/m/s with the insert gradient). However, the gradient switching may cause peripheral nerve stimulation (PNS). PNS is caused by time-varying magnetic fields, as these induce electrical currents in the peripheral nerves. PNS elicits muscle twitching or tingling sensations, which can be unpleasant if sufficiently strong. Since the presented coil is a gradient insert rather than a whole-body gradient system, the PNS threshold is likely obtained at higher slew rates 2. At this time however, the exact PNS threshold for this gradient is still unknown. Since the level of PNS depends on not only the gradient’s amplitude and slew rate, but also on the subject’s anatomy, PNS thresholds vary among subjects 3. Therefore, the goal of this work was to determine the PNS threshold for the 20kHz gradient insert in several subjects.Methods
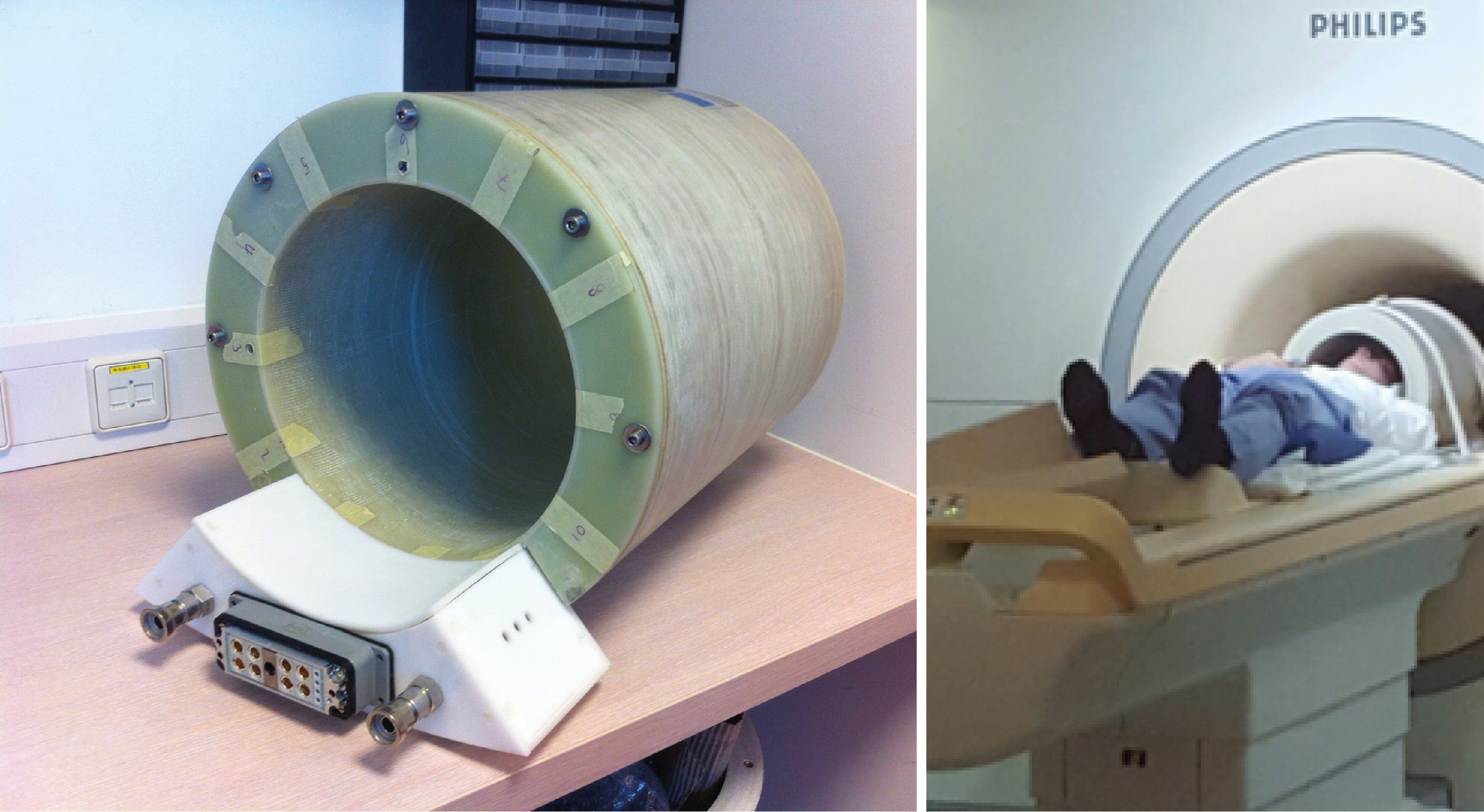
Four healthy subjects participated in this study (3 male, age 29-45). Informed consent was given by all volunteers in accordance to the Institutional Review Board of the UMC Utrecht. All subjects are MRI experts and are familiar with PNS. The experiments were conducted inside the bore of a 7T MRI system (Philips, Best, the Netherlands). The gradient coil is a lightweight (46kg) single-axis (z) head insert (Futura, the Netherlands) and was operated at a fixed frequency of 20.2kHz, driven by an audio amplifier (Powersoft, K20). Figure 1 shows the coil setup. Field camera measurements (Skope, Zürich, Switzerland) were obtained to determine the exact applied fields. The gradient amplitude was varied between 7.5–40mT/m, in 12 steps of 1.25–3.75mT/m. The maximum slew rates for these amplitudes were varied between 952–5076T/m/s. At each amplitude 4 pulse-trains of 50ms were applied, with a pause of 1s between consecutive pulses 4–6. The amplitudes were executed in random order, unknown to the subject, and all amplitudes were repeated. Subjects activated the alarm immediately when they experienced PNS sensations, and indicated the intensity of the sensations on a scale of 1–5 (1 = very mild, 5 = painful). After the measurements the volunteers were asked what sensations they had felt, and if they were able to hear the gradient.Results
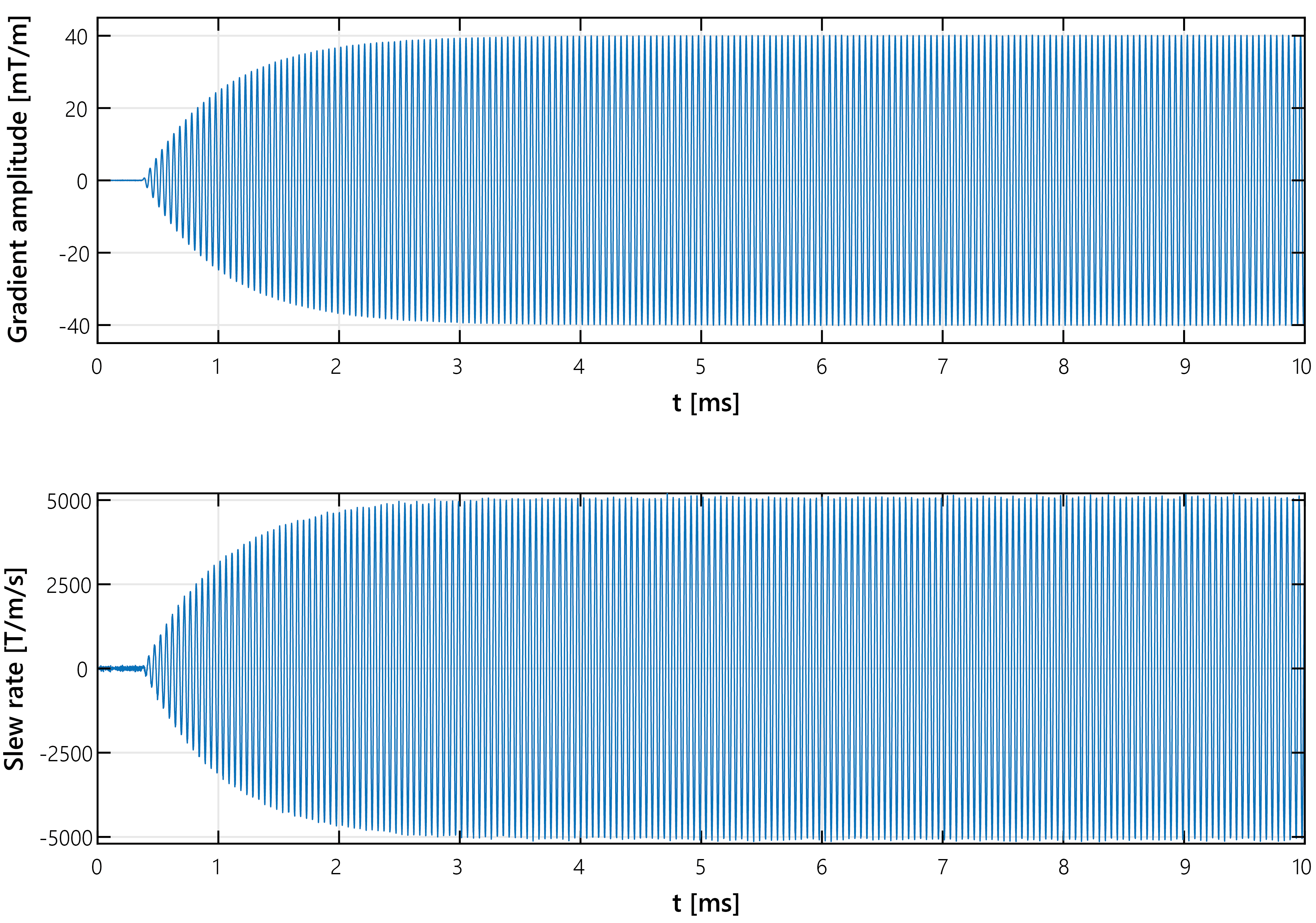
Field cameras confirmed the gradient slew rates up to 5076T/m/s (Figure 2). One subject reported no PNS sensations. One subject reported possible PNS at gradient amplitude 31.25 mT/m during the second repetition only. The subject described this as a very light tingling sensation at the back of the head, but could not distinguish the four distinct pulse trains and expressed doubt whether or not this was PNS. Two subjects reported PNS at gradient amplitudes 36.25mT/m, 37.5mT/m, and 40mT/m. These amplitudes correspond with maximum slew rates during the sinusoidal gradient waveform of 4600T/m/s, 4759T/m/s, and 5076T/m/s, respectively, and average slew rates over the sinusoidal gradient waveform of 2929T/m/s, 3030T/m/s, and 3232T/m/s, respectively. One subject reported PNS during both repetitions of these gradient amplitudes, the other subject reported PNS at the lowest amplitude only during the first repetition. The two subjects described the PNS sensations as a very mild tingling feeling around the teeth, or as a muscle twitching in the left temple. All three subjects reporting PNS described these as mild sensations, rating no more than 1 on the scale of 1–5. All four subjects reported that they were unable to hear the gradient switching.Discussion
Only very mild PNS was observed at the highest slew rates, and not all subjects experienced PNS. This is in line with IEC guidelines that predicts PNS for whole-body gradients at dB/dt slightly above the dB/dt for the head coil, which is approximately 575T/s at a rise time of 12.5µs (corresponding with 20kHz) 7. The sensations at the back of the head reported as possible PNS by the second subject may also be due to the absence of a head cushion. This is supported by the fact that the subject did not report any PNS sensations at other (higher) gradient amplitudes. Higher gradient amplitudes would ideally be included in the study design, in order to determine the PNS threshold in all subjects. This was not possible using the current coil setup due to limitations of the used amplifier, which can generate a maximal gradient strength of 40mT/m at 20kHz, and not by PNS. In future work amplifiers that can generate more power will be used to enable fitting of PNS threshold curves, for instance by stacking more audio amplifiers in parallel, or by increasing the bandwidth of traditional gradient amplifiers.Conclusions
PNS for a 20kHz gradient head coil was measured in four subjects. One subject reported no PNS, two subjects reported mild PNS at the three highest gradient amplitudes, and one subject reported very mild PNS sensations at the fourth highest frequency only. Application of the coil at 20kHz is therefore restricted by the used amplifier, rather than PNS.Acknowledgements
No acknowledgement found.References
1. Versteeg E, Klomp D, Hendrikse J, et al. Supersonic imaging with a silent gradient axis driven at 20 kHz. ISMRM Proc. 2018;4586.
2. Zhang B, Yen Y, Chronik, BA, et al. Peripheral nerve stimulation properties of head and body gradient coils of various sizes. Magn. Reson. Med. 2003;50(1):50–58.
3. Davids M, Guérin B, Malzacher M, et al. Predicting magnetostimulation thresholds in the peripheral nervous system using realistic body models. Sci. Rep. 2017;7:5316.
4. Feldman RE, Hardy CJ, Aksel B, et al. Experimental determination of human peripheral nerve stimulation thresholds in a 3-axis planar gradient system. Magn. Reson. Med. 2009;62:763–770.
5. Lee SK, Mathieu JB, Graziani D, et al. Peripheral nerve stimulation characteristics of an asymmetric head-only gradient coil compatible with a high-channel-count receiver array. Magn. Reson. Med. 2016;76(6):1939–1950.
6. Tan ET, Park KJ, Hua Y, et al. Peripheral nerve stimulation limits of a high amplitude and slew rate magnetic field gradient coil for neuroimaging. 2020;83:352–366.
7. ISO/IEC. NEN-EN-IEC 60601-2-33: Medical electrical equipment - Part 2-33: Particular requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis. ISO/IEC; 2010.
Figures