0096
Fetal whole-heart 4D blood flow MRI with self-calibrated k-t SENSE1School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 2Division of Pediatric Cardiology, The Hospital for Sick Children, Toronto, ON, Canada, 3Department of Congenital Heart Disease, Evelina Children's Hospital, London, United Kingdom
Synopsis
Measurement of blood flow in the fetal heart and the great vessels is challenging due to fetal motion and its small size. Previously, we demonstrated use of k-t SENSE real-time 2D imaging combined with slice-to-volume registration to reconstruct 4D velocity cine volumes. This required 50% of the examination to be spent acquiring training data. In this work we combine sliding window reconstruction of the under-sampled target data with some prior knowledge to dispense with training data altogether. We reconstruct 4D blood flow volumes in 5 fetal hearts using both methods and show that they are broadly equivalent.
Introduction
Quantification of blood flow in the fetal heart and great vessels is very challenging due to its small size and the effects of both fetal and maternal motion. Accelerated acquisition methods such as k-t SENSE [1] can capture the dynamics of the rapidly-beating fetal heart [2] and can be combined with slice-to-volume registration (SVR) motion correction to achieve fetal whole-heart 4D blood flow MRI [3,4]. However, up to half of the scan time during a standard k-t SENSE acquisition is dedicated to collecting training images in order to construct x-f priors for unaliasing the undersampled target data. In this work, which is inspired by self-calibration k-t methods [5], we seek to achieve motion corrected imaging of the fetal heart without using pre-acquired training data, thus reducing acquisition time by 50%.Methods
Imaging was performed on a 1.5T Philips Ingenia scanner. Multi-planar stacks of 2D bSSFP slices were acquired in five pregnant volunteers using the following parameters: TR/TE 3.8/1.9ms, flip angle 60°, 8x k-t SENSE acceleration, field of view 400×304mm, voxel size 2.0×2.0x6.0mm, slice overlap 3-4mm, 96 images per slice. Three fetal hearts were normal, two were diagnosed with congenital abnormalities. All acquisitions included pre-acquired training data and were reconstructed both using this information (standard k-t SENSE) and without it (iterative temporal sliding window k-t SENSE).Self-calibrated k-t SENSE Training Data
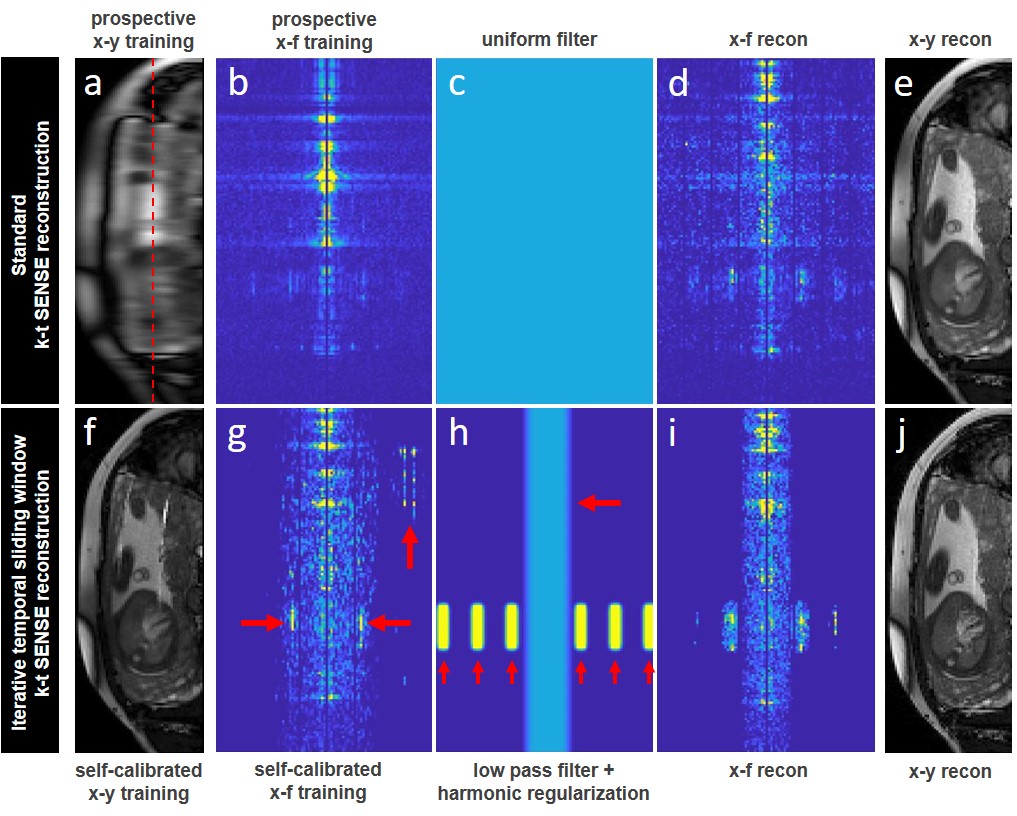
Fig1 shows how x-f space is filtered and regularized using prospective training data in a standard k-t SENSE reconstruction (Fig1a-e), and, using the proposed self-calibrated iterative temporal sliding window k-t SENSE reconstruction method (Fig1f-j). In the new method, a hierarchy of increasingly accelerated k-t reconstruction problems is solved by grouping together the sampled information lying within a temporal sliding window of decreasing widths [8 (= fully sampled), 4, 3, 2, 1, 1]. Within each iteration, the previous reconstruction serves to estimate the x-f signal covariance at the current window size.
Construction of x-f Priors
The reconstruction at the final iteration (Fig1f) satisfactorily recovers low frequencies in x-f space (Fig1g), which are sufficient to capture the maternal dynamics and detect the fetal heart rate (Fig1g, horizontal red arrows). Outside of this low frequency strip, aliases of prominent features remain (Fig1g, vertical red arrow). To create x-f priors that are effective at resolving aliases but retain the full temporal dynamics of the fetal heart, we impose some prior knowledge:
- No high temporal frequency content is expected outside the fetal heart. A Tukey window is employed as a low pass filter to suppress aliases (Fig1h, horizontal red arrow).
- As the fundamental frequency of the fetal heartbeat is identifiable in the self-calibrated training data, its harmonics can also be inferred. Combined with the spatial extent of the fetal heart, this allows priors to be added in the form of Gaussian kernels (3 voxel width) (Fig1h, vertical red arrows) to retain as much temporal information about the heart as possible.
Results
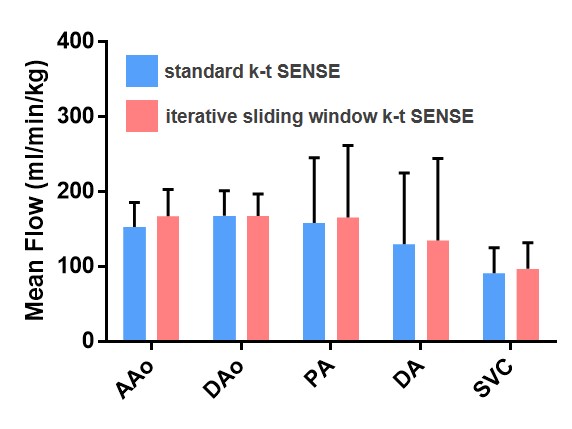
Real-time bSSFP images (Fig2) were spatially and temporally similar between k-t SENSE reconstruction methods in all subjects. Difference images between the two methods showed signal fluctuations across the field-of-view caused by differences in calculation of sensitivities, but the heart region was closely matched for intensity and dynamics. Quantitative evaluation between the two methods was challenging due to subtle differences in the reconstruction frameworks, such as differences due to outlier rejection, and slight misalignment following rigid registration of paired volumes. Visually, 4D magnitude and blood flow velocity cine reconstructions (Fig3 and Fig4) were similar in all five cases. Magnitude volumes were structurally alike and blood flow vectors were directionally consistent. Measurements of mean blood flow through five major vessels (Fig5) were similar between the two methods, with a slightly increased level of flow measured with the iterative sliding window k-t reconstruction.Discussion
The proposed iterative temporal sliding window k-t SENSE reconstruction method allowed for acquisition of real-time 2D bSSFP images without the need for pre-acquired training data. Filtering of x-f space using a low pass filter and knowledge of the harmonic locations of the fetal heartbeat enabled the creation of priors to unalias the undersampled data. Together, these two developments permit a 50% reduction in scan time. This is highly beneficial for fetal cardiac SVR methods as multiple non-coplanar stacks are required for volumetric reconstruction, thus reducing acquisition time for 4D flow measurements from ~14 to ~7 minutes. Reduced scan time also lessens the chance of bulk fetal motion during the examination. For future acquisitions, the scan time gained will be used to increase spatial resolution or acquire more stacks for better estimation of blood flow velocities.Acknowledgements
This work was supported by the Wellcome EPSRC Centre for Medical Engineering at King’s College London (WT 203148/Z/16/Z) and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
[1] Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn. Reson. Med. 2003;50:1031–42.
[2] van Amerom JFP, et al. Fetal cardiac cine imaging using highly accelerated dynamic MRI with retrospective motion correction and outlier rejection. Magn. Reson. Med. 2018;79(1), 327-338.
[3] van Amerom JFP, et al. Fetal whole‐heart 4D imaging using motion‐corrected multi‐planar real‐time MRI. Magn. Reson. Med. 2019;82:1055–1072.
[4] Roberts TA, van Amerom JFP, et al. Fetal whole-heart 4D flow cine MRI using multiple non-coplanar balanced SSFP stacks. (2019) bioRxiv 635797; doi: https://doi.org/10.1101/635797.
[5] Ponce IP, et al. Auto-calibration approach for k-t SENSE. Magn. Reson. Med. 2014;71(3): 1123-1129.
Figures