0090
Fast scan with a wave-CAIPI MPRAGE sequence to minimize motion artifacts in pediatric T1-weighted imaging1Siemens Healthcare Limited, Taipei, Taiwan, 2Department of Medical Imaging, Taipei Medical University Hospital, Taipei, Taiwan, 3Siemens Shenzhen Magnetic Resonance Ltd, Shenzhen, China, 4Siemens Healthineers AG, Erlangen, Germany
Synopsis
Pediatric magnetic resonance imaging (MRI) needs extra care since patients cannot remain still for long in the MRI bore. Therefore, scans should be performed as quickly as possible. Our study investigated the role of fast T1 3D Magnetization Prepared Rapid Acquisition Gradient Echo (MPRAGE) scans using wave-controlled aliasing with parallel imaging (wave-CAIPI) in pediatric patients. We presented that scan times were shortened significantly, and images had fewer motion artifacts compared with conventional MPRAGE images. We further evaluated contrast-to-noise ratios (CNRs) in five cerebellar areas and saw no significant differences between the conventional and wave-CAIPI MPRAGE images.
Introduction
It is difficult for pediatric patients to remain still during magnetic resonance imaging (MRI). Many patients require extra care, such as sedation. In clinical situations, fast scan techniques are often used. Magnetization Prepared Rapid Acquisition Gradient Echo (MPRAGE), a T1-weighted imaging sequence, provides excellent contrast and anatomic cerebral structure to identify pathologic changes. However, this three-dimensional sequence requires longer scan times compared with two-dimensional scans. Recently, wave-controlled aliasing in parallel imaging (wave-CAIPI) MPRAGE was developed, reducing the scan time with only a small g-factor noise penalty [1,2]. Here, we investigated the advantages of using pre- and post-contrast-enhanced wave-CAIPI MPRAGE sequences in pediatric patients to understand whether motion artifacts are suppressed compared with conventional MPRAGE sequences. Furthermore, we assessed contrast-to-noise (CNR) differences between wave-CAIPI MPRAGE and conventional MPRAGE in five different cerebral areas. Statistical analysis was conducted with the Student’s t-test.Methods
Eight pediatric patients were enrolled from 1 to 10 years of age. All scans were performed with a 3T MRI scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) using a 64-channel head-and-neck coil. All patients received MRI scans with conventional MPRAGE and prototype wave-CAIPI MPRAGE sequences. All patients, except one, received contrast-enhanced examinations. The prototype wave-CAIPI MPRAGE sequence modified the conventional gradient echo readouts by playing sinusoidal gradients in phase encoding directions during the sampling period, which leads to a “cork-screw” trajectory [2]. In addition, the two phase-encoding directions are implemented in a 2D CAIPI fashion to further improve g-factor performance and allow for high acceleration [3]. The prototype wave-CAIPI sequence features autocalibration and improved point-spread function (PSF) estimation with joint optimization of the k-space trajectory and parallel imaging reconstruction [4]. Details of the conventional and prototype MPRAGE parameters are compared in Table 1. Images were visually assessed by an experienced radiologist. The scores were set from 0 to 3 (non-diagnostic, poor, adequate, and good, respectively). White and gray matter CNR differences were analyzed in the frontal cortex, temporal cortex, occipital lobe, anterior cingulate cortex, and posterior cingulate cortex. The CNR was measured using contrast-enhanced images from seven patients.Result
Wave-CAIPI provided scan times 3 min shorter than that of conventional MPRAGE (Conventional MPRAGE was 4min 37sec, wave-CAIPI MPRAGE was 1min 33sec). Example images from the wave-CAIPI MPRAGE are shown in Figure 1. No differences in overall image quality were found on the visual assessments, but several cases showed suppressed artifacts with wave-CAIPI (Figure 2). Figure 3 shows representative images from a case where motion artifact was significantly suppressed using wave-CAIPI MPRAGE. Images were plotted to show the signal intensity changes. In conventional MPRAGE imaging, small signal changes in a short distance can be seen because of stripe-like motion artifacts. Wave-CAIPI MPRAGE images showed larger signal intensity changes between white and gray matter. There was one case that showed mild motion artifacts (Figure 4). Furthermore, CNRs were not different between conventional MPRAGE and wave-CAIPI MPRAGE when comparing the frontal cortex, temporal cortex, occipital cortex, anterior cingulate cortex, and posterior cingulate cortex (Figure 5; p>0.05).Discussion
To understand motion artifact effects in conventional and wave-CAIPI MPRAGE images, a signal plot was drawn in the cerebral cortex (Figure 2). Signal differences between white and gray matter were higher in the wave-CAIPI MPRAGE images, which were assumed to represent a lack of motion artifacts since wave-CAIPI MPRAGE scans were captured three times faster than conventional MPRAGE scans. No differences in CNRs were observed in the five cerebral areas examined, with or without contrast enhancement, which suggests that wave-CAIPI MPRAGE can be used similarly to conventional MPRAGE to provide visual diagnostis with shorter acquisition times. We found MPRAGE to have excellent CNRs in white matter, gray matter, and cerebrospinal fluid (CSF) to delineate cerebral structures and detect various pathologies, such as metastatic cerebral tumors. However, MPRAGE requires longer scan times compared with 2D sequences. Since it is difficult for pediatric patients to remain still for long periods, motion artifacts are created that interfere with detecting lesions. Our study suggests that wave-CAIPI MPRAGE T1 3D imaging is superior for pediatric patients in that it can provide stable image quality with fewer motion artifacts. Wave-CAIPI MPRAGE would be beneficial not only to shorten the scan time but to reduce the dose of the sedation for the pediatric examinations.Conclusions
Our study demonstrated that pediatric scans could be acquired three times quicker using a wave-CAIPI MPRAGE sequence compared with a conventional MPRAGE sequence, resulting in greater suppression of motion artifacts. We also showed that the images could be acquired with and without contrast enhancement with no significant differences in CNR.Acknowledgements
No acknowledgement found.References
1. Polak D, Setsompop K, Cauley SF, Gagoski BA, Bhat H, Maier F, Bachert P, Wald LL, Bilgic B. Wave-CAIPI for highly accelerated MP-RAGE imaging. Magn Reson Med. 2018 Jan;79(1):401-406.
2. Bilgic B, Gagoski BA, Cauley SF, Fan AP, Polimeni JR, Grant PE, Wald LL, Setsompop K. Wave-CAIPI for highly accelerated 3D imaging. Magn Reson Med. 2015 Jun;73(6):2152-62.
3. Breuer FA, Blaimer M, Meuller MF, Seiberlich N, Heidemann RM, Griswold MA, Jakob PM. Controlled Aliasing in Volumetric Parallel Imaging (2D CAIPIRINHA). Magn Reson Med. 2006 Mar;55(3):549-56.
4. Cauley SF, Setsompop K, Bilgic B, Bhat H, Gagoski B, Wald LL. Autocalibrated wave-CAIPI reconstruction; Joint optimization of k-space trajectory and parallel imaging reconstruction. Magn Reson Med 2016. Sep;78(3):1093-1099.
Figures
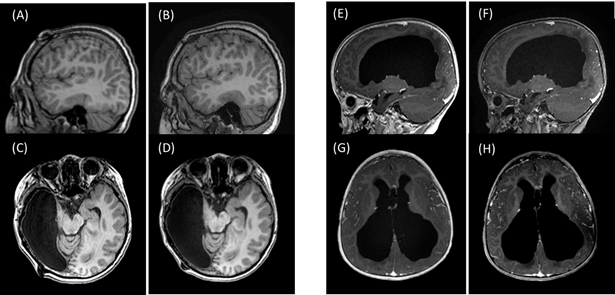
Figure 1. Representative images from pediatric patients scanned with conventional MPRAGE (A, C, E, G) and wave-CAIPI MPRAGE (B, D, E, F) with and without contrast enhancement. The left images (A–D) are without contrast enhancement from a 9-year-old patient, and the right images (E–F) are with contrast enhancement from a 3-year-old patient.
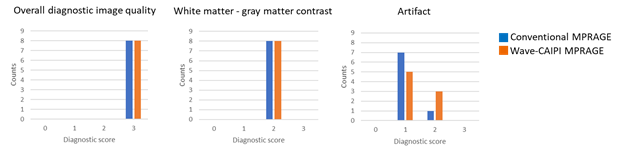
Figure 2. A visual assessment of conventional MPRAGE and wave-CAIPI MPRAGE images. The diagnostic score was set from 0 to 3, for which 3 was designated the best image quality. Overall image quality did not change between the two MPRAGE images, but the artifact was decreased in wave-CAIPI MPRAGE images.
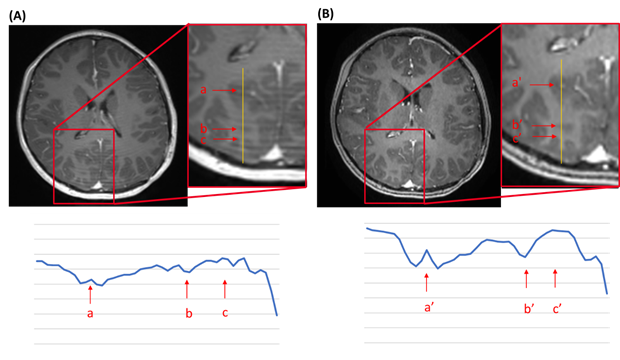
Figure 3. An 8-year-old pediatric patient scanned with both conventional MPRAGE (A) and wave-CAIPI MPRAGE (B) with contrast enhancement. Magnified regions are present on the right side of each image. The bottom plot shows the signal intensities of the yellow line marked in the magnified images. Motion artifacts in (A) caused the frequent signal changes observed as stripe artifacts in the cortex. Motion artifacts were suppressed in (B), allowing for a clear difference between signal intensities in the white and gray matter.
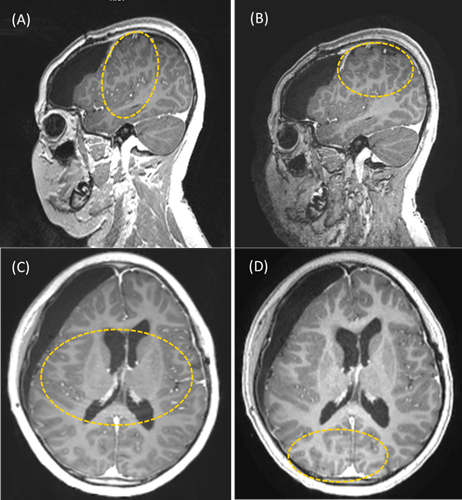
Figure 4. An 11-year-old patient with motion artifacts on the conventional MPRAGE images (A and C). Motion artifacts were still observed on the wave-CAIPI MPRAGE images but were milder (B and D). The yellow dotted ellipses show the areas where the artifacts can be observed.
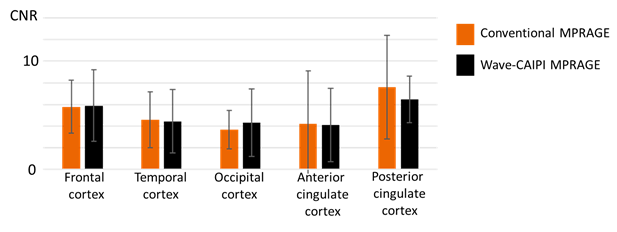
Figure 5. Contrast-to-noise ratio (CNR) of white and gray matter in five different cerebral regions. No significant differences in CNR were seen in any of the regions between the conventional MPRAGE and wave-CAIPI MPRAGE images.