0087
Assessment of Free-Breathing Radial Magnetic Resonance Elastography in Healthy Children and Children with Liver Disease at 3T1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3Diagnostic Imaging, St. Jude Children’s Research Hospital, Memphis, TN, United States, 4Pediatrics, University of California, Los Angeles, Los Angeles, CA, United States, 5Siemens Medical Solutions, Salt Lake City, UT, United States
Synopsis
Hepatic stiffness measured by magnetic resonance elastography (MRE) is a biomarker that correlates with histopathological staging of liver fibrosis. Conventional Cartesian gradient-echo MRE requires breath-holding (BH), which may be inconsistent and challenging for children. Free-breathing (FB) MRE based on radial acquisition is a promising solution to this problem. In this study, we investigated the agreement in hepatic stiffness values from BH-MRE and FB-MRE, as well as repeatability, in healthy children and pediatric patients at 3T. Bland-Altman analysis showed a high level of agreement between BH-MRE and FB-MRE, and repeatability analysis showed similar performance for BH-MRE and FB-MRE.
Introduction
Magnetic resonance elastography (MRE) accurately measures hepatic stiffness, which correlates with histopathological fibrosis staging [1-4] and is a promising biomarker to detect and classify liver fibrosis [1-6]. However, conventional gradient-echo (GRE) MRE sequences based on Cartesian sampling require multiple breath-holds (BH), which may be impractical, especially in children, due to inconsistencies between multiple BHs or inability to perform breath-holding [7-8]. Radial free-breathing (FB) GRE MRE has been recently developed to overcome this problem, with promising initial feasibility demonstrated at 1.5T [9]. Previous studies have not yet assessed the accuracy and repeatability of radial FB-MRE, nor its performance at 3T. In this study, we investigated the agreement and repeatability of hepatic stiffness measurements from Cartesian BH-MRE and radial FB-MRE at 3T in healthy children and pediatric patients with liver disease.Methods
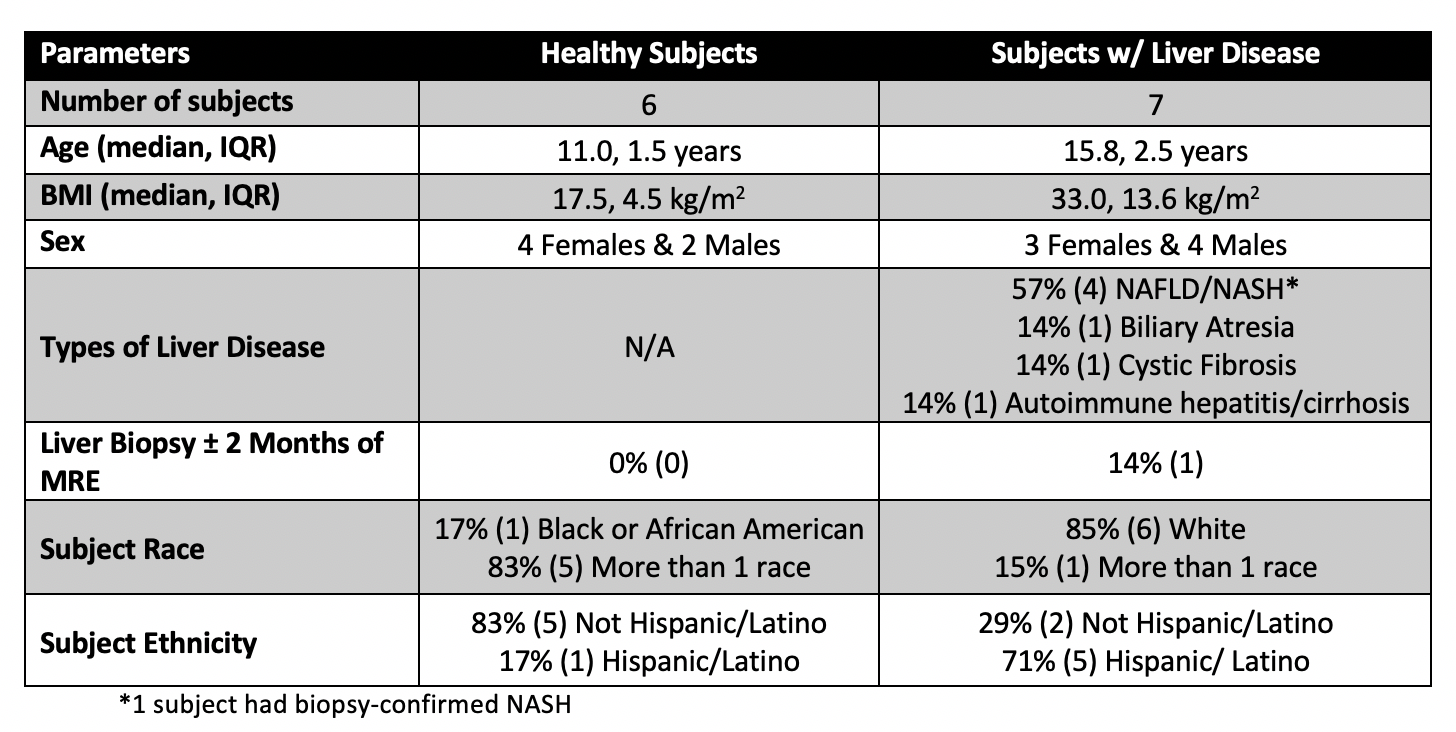
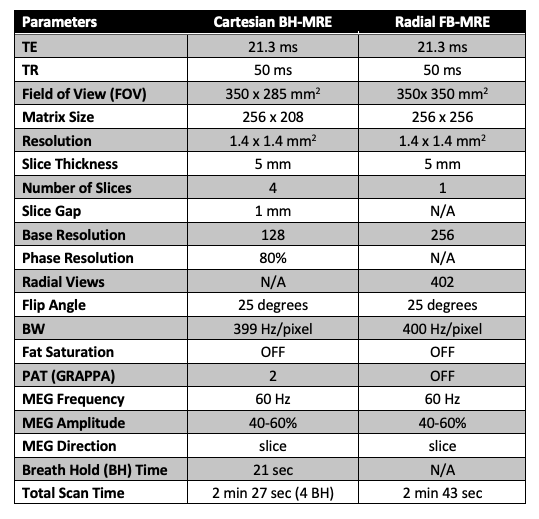
MRE Acquisition: 6 healthy children and 7 pediatric patients with liver diseases were enrolled in this IRB-approved HIPAA-compliant study (Table 1). To assess repeatability, a Cartesian BH-MRE sequence and a prototype radial FB-MRE sequence were each acquired twice in the same exam at 3T (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). Table 2 lists the Cartesian BH-MRE and radial FB-MRE parameters, which were matched as much as possible. Due to time constraints, only 2 slices were acquired with radial FB-MRE. These 2 slices were chosen to match the slice positions with the largest measurable liver region-of-interest (ROI) size in the Cartesian BH-MRE stiffness maps, as determined by the numerical confidence interval (CI) maps [10]. Two matched slices from all subjects were used for analyses. All of the MRE images and stiffness maps were reconstructed using the scanner software.Analysis: Using custom software (MATLAB, Mathworks, MA, USA), hepatic stiffness was measured in ROIs inside the liver with ≥90% CI. The within-technique mean and standard deviation (SD) of hepatic stiffness were calculated for Cartesian BH-MRE and radial FB-MRE, which were each acquired twice. Repeatability was assessed in terms of the within-technique coefficient of variation (CoV = SD/mean). Agreement in the within-technique mean stiffness measurements between Cartesian BH-MRE and radial FB-MRE was evaluated using Bland-Altman analysis in terms of the mean difference (MD) and 95% limits of agreements (LoA).
Results
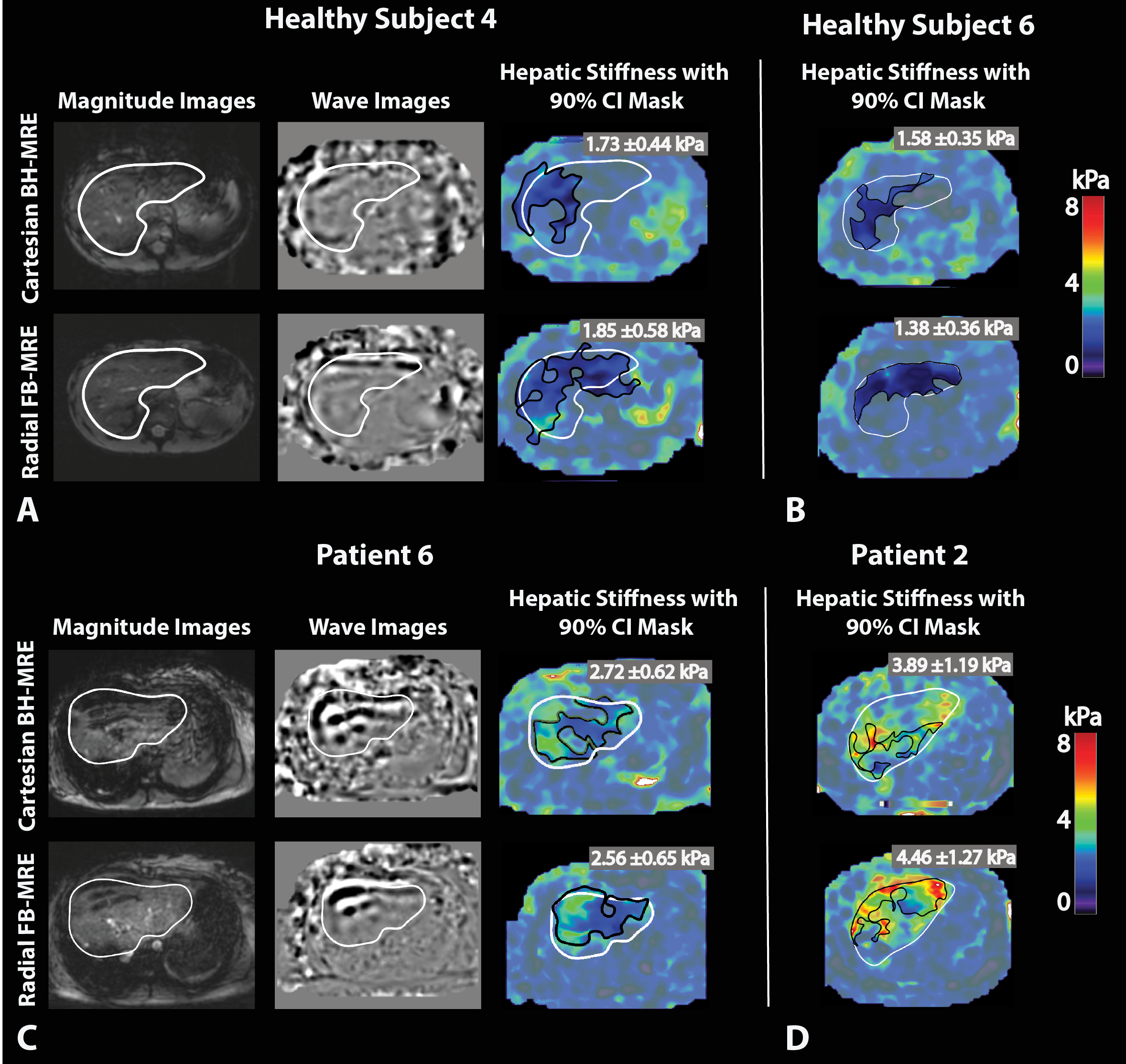
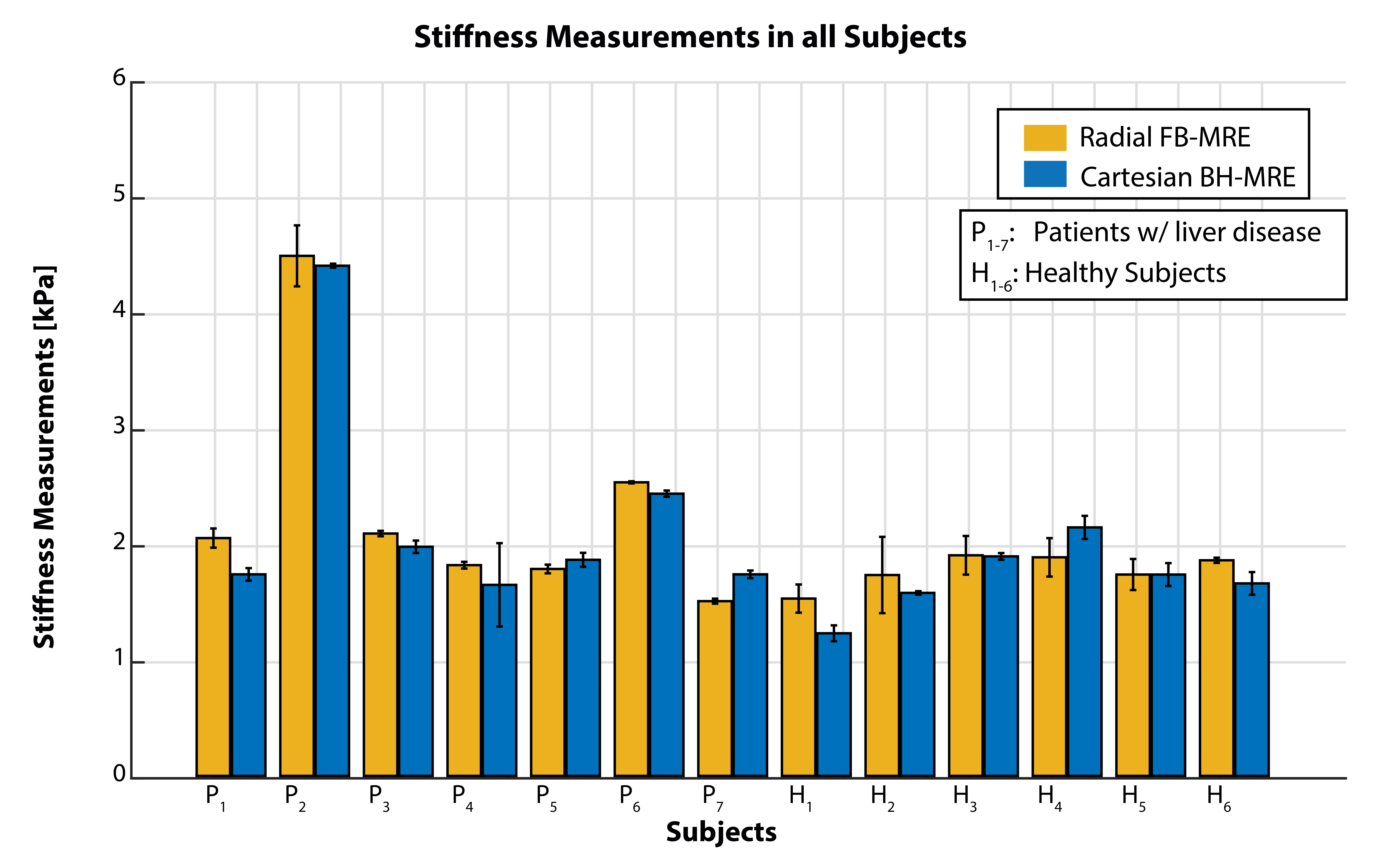
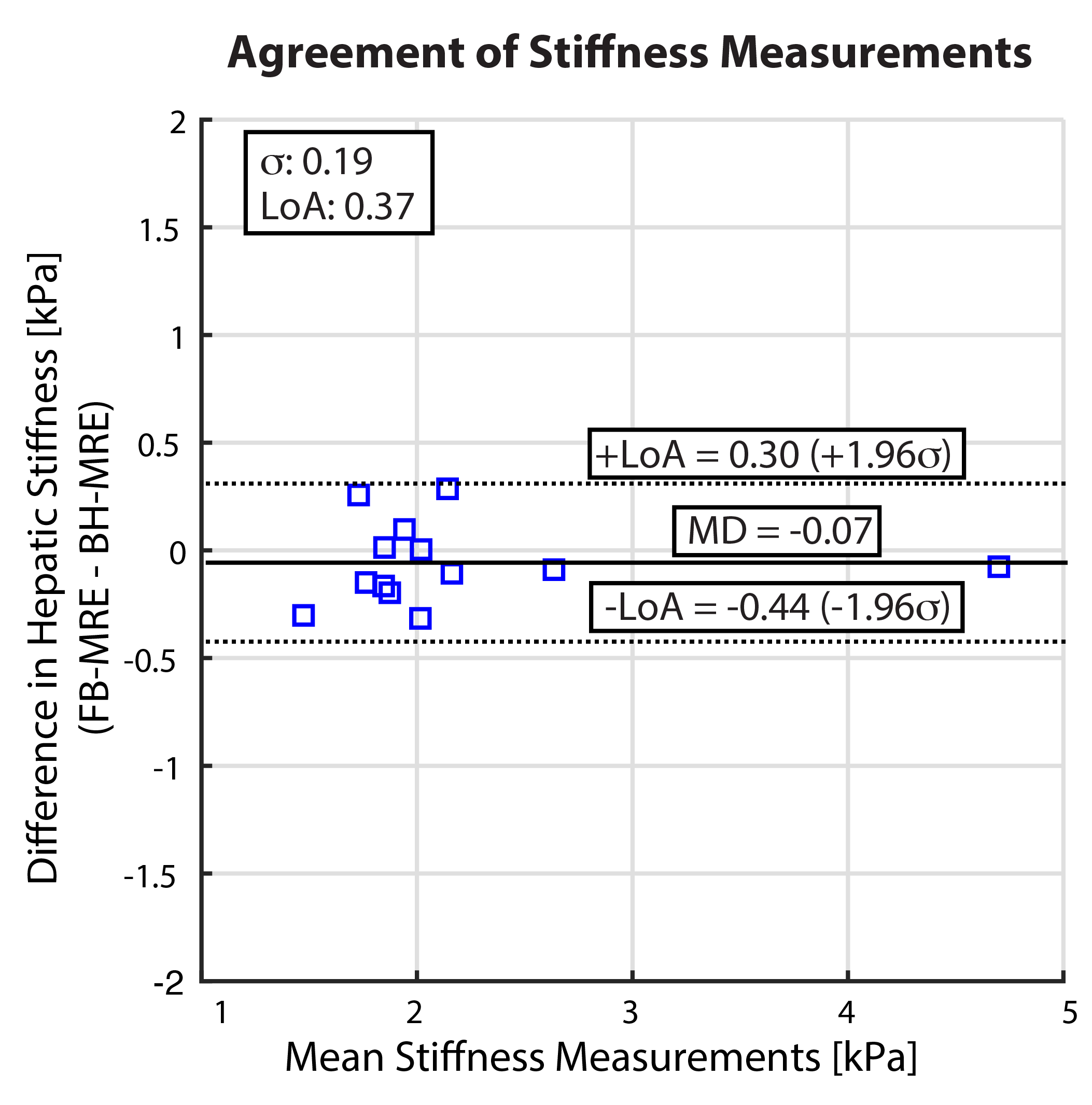
The MRE magnitude images, wave images, and stiffness maps with 90% CI and liver contours are shown in Fig. 1 for representative healthy subjects and patients. In these examples, the stiffness maps from radial FB-MRE had comparable or larger measurable ROI sizes vs. Cartesian BH-MRE.Cartesian BH-MRE and radial FB-MRE yielded similar within-technique mean and SD of hepatic stiffness values for all subjects (Fig. 2). The hepatic stiffness measurements in healthy subjects were consistent with stage 0 fibrosis [11]. Patient 2 shown in Fig. 1D had biopsy-confirmed steatohepatitis and cirrhosis, consistent with the hepatic stiffness values measured by BH-MRE and FB-MRE. For the other patients, the hepatic stiffness measurements from BH-MRE and FB-MRE were consistent with each other. From Bland-Altman analysis, LoA = [-0.44, 0.30] kPa and MD = -0.07 kPa (Fig. 3). CoV [median, interquartile range] was [0.029, 0.048] for Cartesian BH-MRE and [0.022, 0.030] for radial FB-MRE across the healthy subjects and pediatric patients, indicating a similar level of repeatability.
Discussion
A previous study assessed the feasibility of radial FB-MRE at 1.5T in 2 healthy subjects and 2 patients with ages ranging from 14 to 52 years [9]. Here, we assessed radial FB-MRE at 3T with an increased number of subjects, and specifically in healthy children and pediatric patients with liver diseases. Cartesian BH-MRE and radial FB-MRE yielded similar within-technique mean, SD, and CoV for hepatic stiffness, indicating similar quantification results and repeatability. Hepatic stiffness values from Cartesian BH-MRE MRE and radial FB-MRE agreed with each other with low MD.There were some limitations to our study. Due to the longer acquisition time of the current radial FB-MRE technique (2 min 43 sec per slice; Table 2), only 2 slices were acquired because of time constraints. For future work, simultaneous-multi-slice imaging [12-13] and rapid GRE MRE encoding strategy could be used to accelerate radial FB-MRE [14]. Radial FB-MRE may also benefit from gradient calibration [15] and self-navigated motion compensation [9,16-17], which have improved quantitative FB liver MRI and MRE. Finally, more patients with liver diseases should be studied to cover a wider range of hepatic stiffness values.
Conclusion
In this study, radial FB-MRE was shown to be repeatable and in agreement with Cartesian BH-MRE in healthy children and pediatric patients at 3T. Radial FB-MRE is a promising technique for hepatic stiffness measurements in children when breath-holding is challenging or impractical.Acknowledgements
This study was supported in part by an Exploratory Research Grant from the UCLA Department of Radiological Sciences. The authors thank Dr. Joanna Yeh, the study coordinators, and MRI technologists at UCLA.References
1] Venkatesh, Sudhakar K., Meng Yin, and Richard L. Ehman. "Magnetic resonance elastography of liver: technique, analysis, and clinical applications." Journal of magnetic resonance imaging 37.3 (2013): 544-555.
[2] Batheja, Mashal, et al. "Magnetic resonance elastography (MRE) in assessing hepatic fibrosis: performance in a cohort of patients with histological data." Abdominal imaging 40.4 (2015): 760-765
[3] Xanthakos, Stavra A., et al. "Use of magnetic resonance elastography to assess hepatic fibrosis in children with chronic liver disease." The Journal of pediatrics 164.1 (2014): 186-188.
[4] Singh, Siddharth, et al. "Diagnostic performance of magnetic resonance elastography in staging liver fibrosis: a systematic review and meta-analysis of individual participant data." Clinical Gastroenterology and Hepatology 13.3 (2015): 440-451.
[5] Yin, Meng, et al. "Hepatic MR elastography: clinical performance in a series of 1377 consecutive examinations." Radiology 278.1 (2015): 114-124.
[6] Kim, Yong Seek, Yu Na Jang, and Ji Soo Song. "Comparison of gradient-recalled echo and spin-echo echo-planar imaging MR elastography in staging liver fibrosis: a meta-analysis." European radiology 28.4 (2018): 1709-1718.
[7] Murphy, Ian Gavin, et al. "Comparison of breath-hold, respiratory navigated and free-breathing MR elastography of the liver." Magnetic resonance imaging 37 (2017): 46-50.
[8] Hines, Catherine DG, et al. "Repeatability of magnetic resonance elastography for quantification of hepatic stiffness." Journal of Magnetic Resonance Imaging 31.3 (2010): 725-731.
[9] Holtrop, Joseph et al. “Free Breathing Radial Magnetic Resonance Elastography” Proc. Int. Soc. Magn. Reson. Med. 27th. p 4482 (2019).
[10] Felker, Ely R., et al. "Liver MR Elastography at 3 T: Agreement Across Pulse Sequences and Effect of Liver R2* on Image Quality." American Journal of Roentgenology 211.3 (2018): 588-594.
[11] Venkatesh, Sudhakar Kundapur, and Richard L. Ehman. "Magnetic resonance elastography of liver." Magnetic Resonance Imaging Clinics 22.3 (2014): 433-446.
[12] Adluru, Ganesh, et al. "Radial simultaneous multi slice imaging for rapid cardiac imaging." Journal of Cardiovascular Magnetic Resonance 18.S1 (2016):
[13] Yutzy, Stephen R., et al. "Improvements in multislice parallel imaging using radial CAIPIRINHA." Magnetic resonance in medicine 65.6 (2011): 1630-1637.
[14] Chamarthi, Suresh K., et al. "Rapid acquisition technique for MR elastography of the liver." Magnetic resonance imaging 32.6 (2014): 679-683.
[15] Armstrong, Tess, et al. "Free‐breathing liver fat quantification using a multiecho 3 D stack‐of‐radial technique." Magnetic resonance in medicine 79.1 (2018): 370-382.
[16] Armstrong, Tess, et al. "Free-breathing fat quantification in the liver using a multiecho 3D stack-of-radial technique: investigation of motion compensation and quantification accuracy." Proc. Int. Soc. Magn. Reson. Med. 25th. p 363 (2017).
[17] Zhong, Xiaodong, et al. “Effect of Respiratory Motion on Free-Breathing Three- Dimensional Stack-of-Radial Liver R2 * Relaxometry and Improved Quantification Accuracy Using Self-Gating.” Magnetic Resonance in Medicine. In Press (2019)
Figures