0062
In vivo proton exchange rate mapping is highly correlated with Gadolinium enhancement for staging Multiple Sclerosis Lesions1Radiology, Tongji hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2Radiology, University of Illinois at Chicago, Chicago, IL, United States, 3Center for MR Research, University of Illinois at Chicago, Chicago, IL, United States, 4Bioengieering, University of Illinois at Chicago, Chicago, IL, United States
Synopsis
In this study, at the first time, we performed in vivo kex MRI of MS patients and evaluated its potential value for staging clinical MS lesions. In vivo proton exchange rate mapping was found to be highly correlated with Gadolinium enhancement for determining lesion activity. With further validation, kex may be an alternative endogenous MRI contrast for the clinical determination of dissemination in time (DIT) of MS lesions.
Background and Purpose:
Multiple sclerosis (MS) is a leading cause of neurologic disability in young adults. As one of the high priority areas for MS research by the latest 2017 McDonald criteria1, the determination of dissemination in time (DIT) highly relies on repeated Gadolinium (Gd)-enhanced MRI. However, Gd-enhanced MRI is proven to have a few limitations, including the risks for patients with renal failure2 and the Gd accumulation in brain3. Therefore, MRI methods based on endogenous contrast will be highly desirable.In vivo proton exchange rate (kex) imaging of brain based on water direct saturation (DS) removed omega plot4 has been implemented for healthy subjects4,5. As a novel imaging contrast, endogenous kex may help for the risk stratification of neurological diseases, predicting prognosis, and guiding treatment strategies. In this study, at the first time, we performed in vivo kex MRI of MS patients and evaluated its potential value for staging clinical MS lesions.
Materials and Methods:
Under approved IRB protocols, sixteen consecutive MS patients (7M/9F, aged 18-50 years, EDSS 0-6.5, disease duration 1-12years) were included. Conventional MRI including post-contrast T1-weighted imaging and single-slice CEST imaging were performed on a 3.0T GE MR750 scanner. Sequence parameters of CEST were as follows: TR/TE = 3000/22.6ms, field of view= 24 × 24 cm2, matrix = 128 × 128, slice thickness = 5 mm, NEX = 2, CEST saturation power = 1,2,3,4&5μT,saturation duration=1.5 s, and 33 frequency offsets ranging from -6 to +6 ppm, +15.6 & +39.1 ppm. kex maps were generated based on DS-removed omega plots 6. MS lesions with T2 hyperintensity were assessed for Gd enhancement and kex signal elevation compared to normal appearing white matter (NAWM). Two-tailed student’s t test was used for analyzing the statistical difference of kex values between lesions and NAWM with statistical significance set at 0.05.Results:
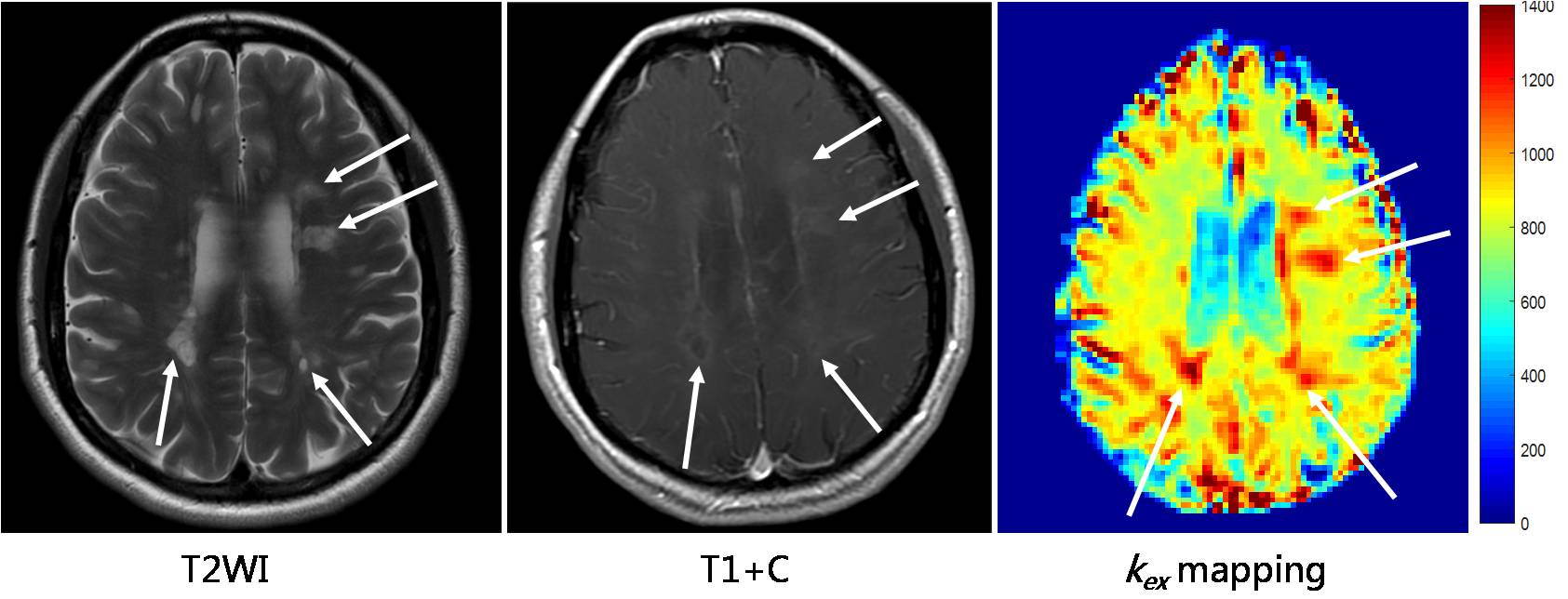
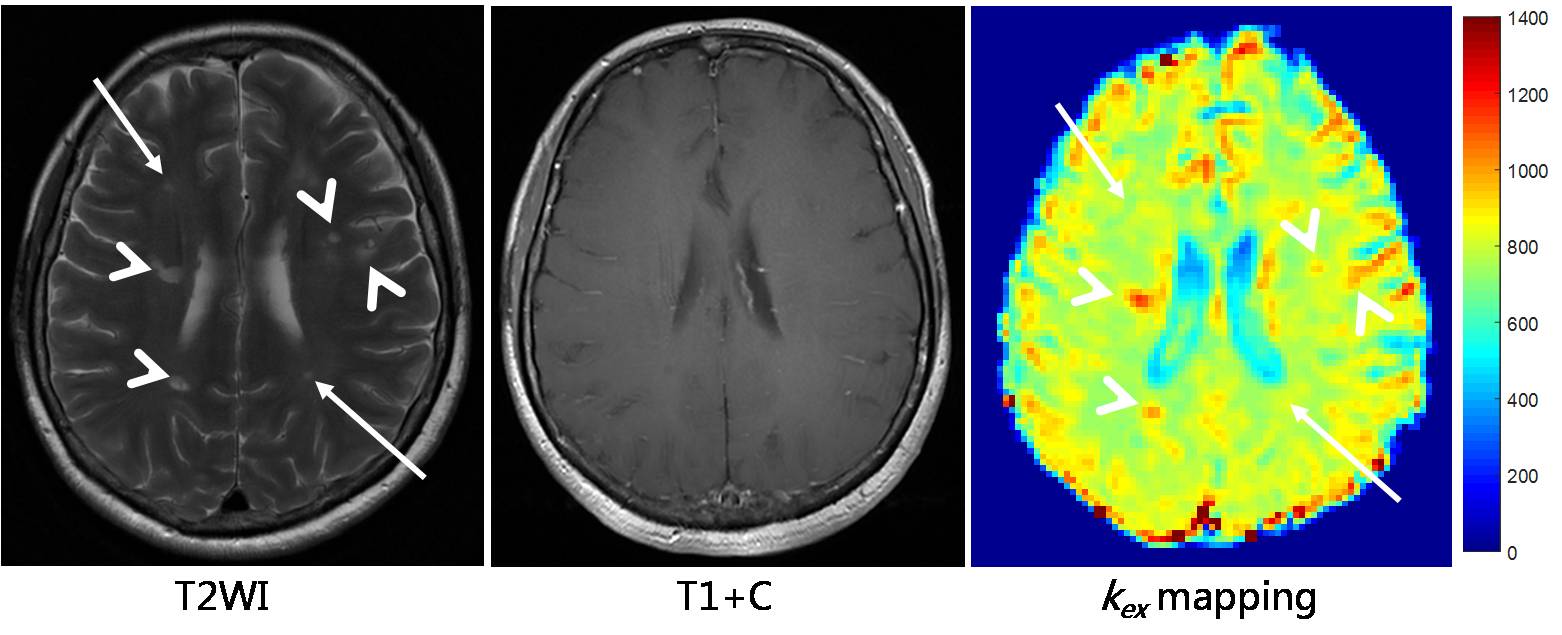
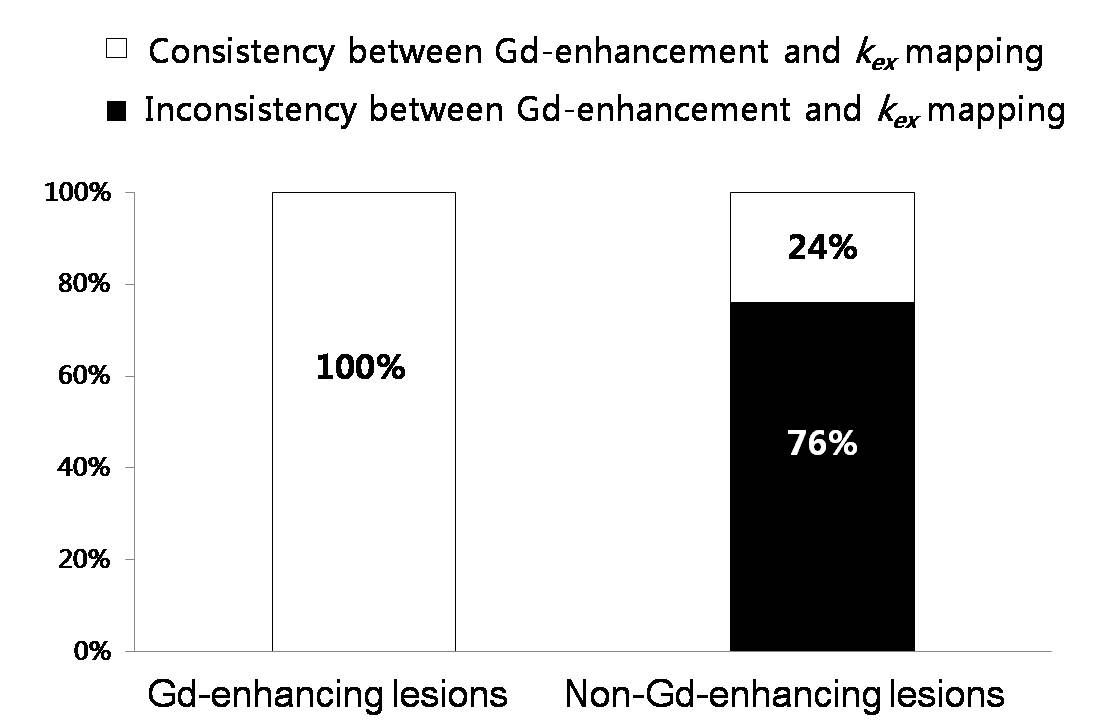
In all Gd-enhanced lesions (51% of the 153 total MS lesions or 78), kex maps showed elevated signal by 27±14% (p<0.0001) compared to NAWM. There is no case in which there is Gd-enhancement while on kex signal elevation was not detected. In non-Gd-enhanced lesions (49% of the 153 or 75), 18 lesions showed no kex elevation and 57 showed kex elevation by 27±13% (p<0.0001) compared to NAWM. Overall, kex mapping showed consistency with Gd-enhancement in 62.7% of lesions; in the rest 37.3% of lesions, kex MRI appears to show higher sensitivity in detecting lesion activity than Gd-enhancement MRI. Given that it is known that Gd-enhanced MRI often provides false negative results, the activity of these 37.3% of lesions is to be verified with other clinical data and/or other MRI modality such as Quantitative Susceptibility Mapping.Discussion and conclusion:
Our preliminary data demonstrated that kex MRI is highly correlated to Gd-enhanced contrast maps by showing elevated kex from all Gd-enhanced lesions. Our previous studies6 found reactive oxygen species (ROS) to be a specific factor for elevated tissue kex in vivo when pH and temperature is not changing, such as in MS lesions. Elevated ROS production in active and inflammatory lesions may explain the correlation between kex mapping and Gd enhancement, both indicating lesion activity. With further validation, kex may be an alternative endogenous MRI contrast for the clinical determination of DIT of MS lesions.Acknowledgements
No acknowledgement found.References
1. Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162-73.
2. Perazella MA. Current status of gadolinium toxicity in patients with kidney disease. Clin J Am Soc Nephrol. 2009;4(2):461-9.
3. Kanda T, Ishii K, Kawaguchi H, et al. High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose of a gadolinium-based contrast material. Radiology. 2014;270(3):834-41.
4. Dixon WT, Ren J, Lubag AJ, et al. A concentration-independent method to measure exchange rates in PARACEST agents. Magnetic resonance in medicine. 2010;63(3):625-32.
5. Shaghaghi M, Chen W, Scotti A, et al. In vivo quantification of proton exchange rate in healthy human brains with omega plot. Quant Imaging Med Surg. 2019.
6. Tain RW, Scotti AM, Cai K. Improving the detection specificity of endogenous MRI for reactive oxygen species (ROS). JMRI. 2019;50(2):583-91.
Figures