0036
T1 and T2 relaxometry of arterial and venous blood: reliability of different methods1Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 2Biomedical Engineering & Physics, Amsterdam UMC, Amsterdam, Netherlands
Synopsis
We investigated the reliability of different T1 and T2 relaxometry methods for arterial and venous blood. While TRIR enables measurements of both venous blood T1 and T2, T2 estimates from TRIR showed poorer repeatability compared to TRUST. Moreover, significantly higher venous blood T2 values were observed using TRIR. Lastly, arterial blood T1 measurements showed a better repeatability compared to venous T1 measurements using TRIR. These findings advocate for the use of the arterial T1 measurements instead of venous T1 and the use of TRUST to measure venous blood T2.
Introduction
T1 and T2 relaxometry measurements of arterial and venous blood are of great importance in a number of neurovascular applications. Specifically, arterial T1 is used in the quantification of cerebral blood flow (CBF) using arterial spin labeling (ASL)1, while from venous T2, blood oxygenation can be derived.2 Several MRI sequences have been proposed to measure arterial and venous blood T1 and T2 relaxation rates. Li et al.3 described a method for fast measurements of arterial T1, while venous T2 is commonly measured using T2 Relaxation Under Spin Tagging (TRUST).2 Another method, T2-prepared blood Relaxation Imaging with Inversion Recovery (TRIR) combines venous T2 and T1 quantification in one sequence4 by acquiring multiple inversion recovery curves with different T2 preparations. T1 and T2 estimates from these methods should be reliable before incorporating them as prior knowledge in quantitative perfusion and oxygenation estimation. Therefore, we investigated the intra- and inter-session repeatability of these three (arterial T1 / TRUST / TRIR) techniques and possible bias between TRUST and TRIR measurements of venous T2.Methods
Eight healthy volunteers (four female, 28 ± 9 years old) underwent two scan sessions (see Figure 1), on a Philips 3T Ingenia system using a 32-channel head coil. Between sessions, volunteers were repositioned on the MRI table. Three TRUST and TRIR measurements per session were performed in an interleaved fashion to assess venous blood T1 and T2 in the sagittal sinus. Additionally, arterial blood T1 was measured three times per session in the carotid arteries using the sequence described by Li et al.3 These measurements required changing the position of the volunteers to achieve homogenous inversion efficiency from the heart to the ICA, and were therefore performed in consecutive order. All scans were performed and post-processed as described in previous work.2-4 For intra-session repeatability assessment, Bland-Altman analysis was performed by comparing all possible combinations of within-session repeated scans. For inter-session repeatability, measurements in both sessions were compared pairwise. Using the same combinations, coefficients of variation (CV) were calculated as the ratio of the standard deviation of the difference between the repeated measurements over the mean of all measurements.Results
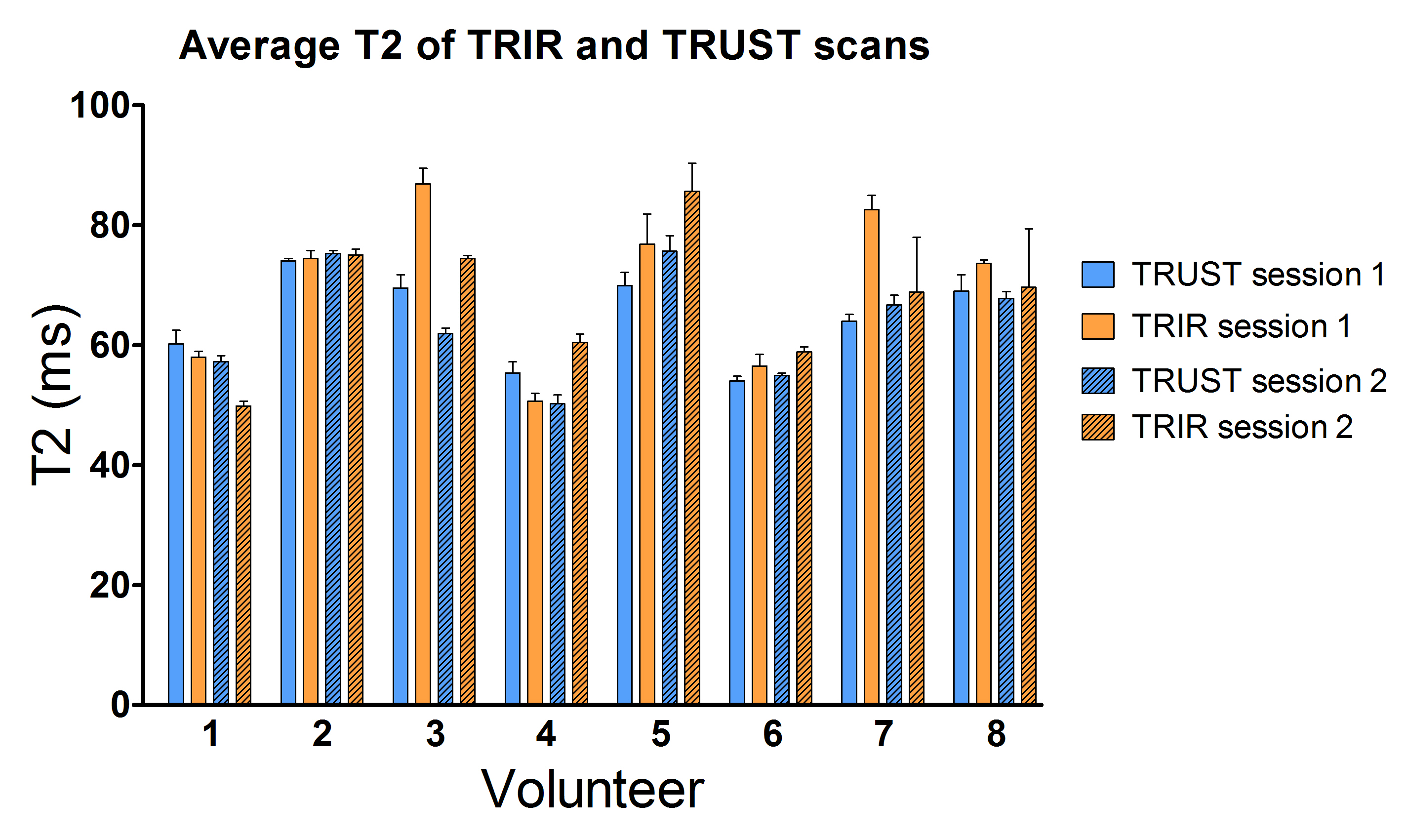
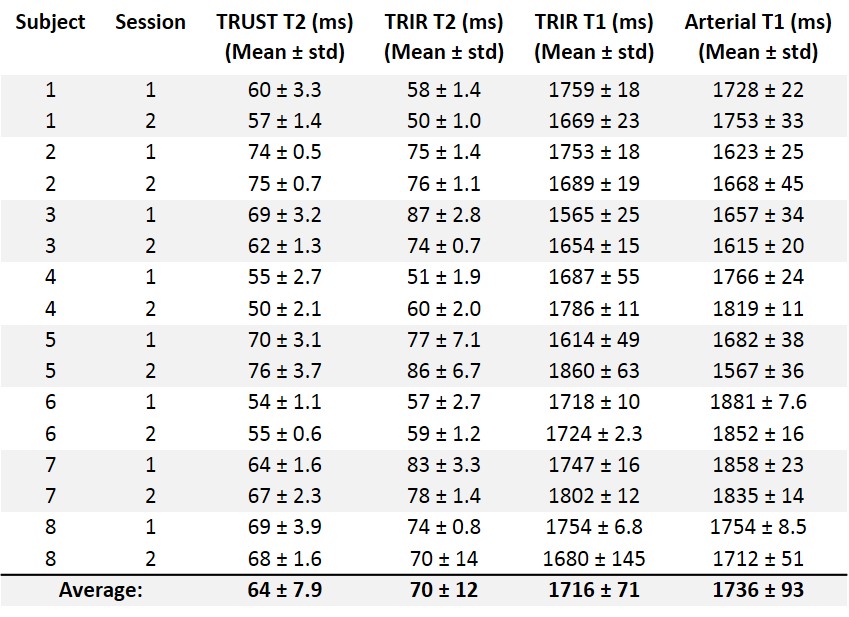
Representative TRUST, TRIR and arterial T1 scans together with their corresponding fits are shown in Figure 2. For venous blood T2 measurements, confidence interval widths of the T2 estimates, expressed as a percentage of the fitted value, were 14 ± 12% and 3.7 ± 1.0% for TRUST and TRIR respectively. For venous (from TRIR) and arterial T1 measurements, confidence intervals of the T1 estimates were 3.0 ± 0.7% and 7.5 ± 2.8%, respectively.Mean values of TRUST and TRIR based venous blood T2 values for each volunteer and session are shown in Figure 3 (also see Table 1). TRIR measurements resulted in significantly higher (p < 0.05) T2 values as compared to TRUST (70.1 ± 12.7 vs. 64.1 ± 8.2). Bland-Altman plots of intra- and intersession repeated measurements are shown in Figure 4. For all scans, the intra- and inter-session bias was close to zero. Both intra-session and inter-session CV values were poorer for TRIR (9.2% / 9.2%) as compared to TRUST (3.9% / 4.4%). Note that for both methods, intra- and inter-session repeatability was similar. Finally, venous T1 measurements from TRIR also had slightly poorer intra- and inter-session repeatability (CV values: 3.7% / 4.8%), as compared to arterial T1 measurements (CV values: 1.6% / 2.5%).
Discussion and Conclusion
While TRIR acquisitions have the benefit of quantifying both T1 and T2 of venous blood, our data suggests that the TRIR overestimates venous blood T2 values compared to the more commonly used TRUST sequence. Moreover, TRIR results in poorer intra- and inter-session repeatability of T1 and T2 estimates compared to the alternative methods (TRUST and arterial T1), with our CV values of arterial T1 corresponding well to data from Li et al.3 Although T2 estimates from TRIR had lower repeatability as compared to TRUST, the confidence intervals of the fits were lowest in case of TRIR. Whether this originates from biases created by the simultaneous fit or a factor from the sequence itself is currently being investigated. Overall, our findings advocate for the use of the arterial T1 measurements instead of venous T1 (e.g. for CBF quantification in ASL) and the use of TRUST to measure venous blood T2 from which oxygenation and oxygen extraction fraction can be derived.Acknowledgements
No acknowledgement found.References
1. Alsop DC, Detre JA, Golay X, Günther M, Hendrikse J, Hernandez‐Garcia L, Lu H, MacIntosh BJ, Parkes LM, Smits M, Van Osch MJ. Recommended implementation of arterial spin‐labeled perfusion MRI for clinical applications: a consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magnetic resonance in medicine. 2015 Jan;73(1):102-16.
2. Lu H, Ge Y. Quantitative evaluation of oxygenation in venous vessels using T2‐relaxation‐under‐spin‐tagging MRI. Magnetic Resonance in Medicine. 2008 Aug;60(2):357-63.
3. Li W, Liu P, Lu H, Strouse JJ, van Zijl PC, Qin Q. Fast measurement of blood T1 in the human carotid artery at 3T: Accuracy, precision, and reproducibility. Magnetic resonance in medicine. 2017 Jun;77(6):2296-302.
4. Petersen, E.T., De Vis, J.B., Alderliesten, T., Kersbergen, K.J., Benders, M.J.N.L., Hendrikse, J., van den Berg, N. Simultaneous OEF and haematocrit assessment using T2 prepared blood relaxation imaging with inversion recovery. Proceedings International Society of Magnetic Resonance in Medicine. 2012 20, 472
Figures