0024
Optimization of Pseudo-Continuous Arterial Spin Labeling using Off-resonance Compensation Strategies at 7T1NINDS/LFMI, National Institutes of Health, Bethesda, MD, United States, 2NINDS/NMRF, National Institutes of Health, Bethesda, MD, United States
Synopsis
Pseudo-continuous arterial spin labeling (PCASL) is very sensitive to off-resonance effects. This is especially a problem at higher fields (>3T). Off-resonance effects can be compensated by using an average or a vessel-specific correction integrated into the PCASL tagging/control pulse. Vessel-specific corrections can be performed using a prescan or a field map. In this study, we compared three off-resonance compensation strategies at 7T. Data showed that a large improvement (> 2 times) of the PCASL signal can be obtained with subject specific off-resonance correction with all 3 methods. The field map based method showed slightly better performance over the others.
Introduction
Pseudo-continuous arterial spin labeling (PCASL) is an established pulse sequence for perfusion MRI1. It is well known that off-resonance effects can cause significant degradation of the PCASL tagging efficiency deteriorating the image quality and the cerebral blood flow estimation2,3. Robustness of PCASL to off-resonance effects can be increased by using an unbalanced PCASL scheme, a short RF separation, a low average gradient, a low selective/average gradient ratio, and a high B14,5. However, these solutions can be hard to optimize, especially at high-field (>3T) where SAR restrictions and off-resonance effects are heightened6,7.To compensate for these effects an optimal PCASL RF phase increment can be calculated either by a pre-scan procedure6 or an off-resonance field ($$$\triangle$$$B0) map of the tagging location8,9. In the pre-scan approach, a series of low-resolution perfusion images of one or more slices is acquired with different PCASL RF phase increments. When using the field map method, the average off-resonance field and the off-resonance gradient are determined at the tagging plane, directly around the feeding arteries.
A more comprehensive approach consists of compensating for in-plane off-resonance by combining the PCASL RF phase increment with appropriate transverse gradients. In this case, instead of using an average off-resonance correction, small in-plane rephasing gradients are calculated based on the spatial information derived either from the prescan or the field map6. In this work, we compare the effectiveness of using vessel-specific and an average off-resonance correction to optimize PCASL imaging at 7T.
Methods
Five healthy volunteers (3 men and 2 women, age 26$$$\pm$$$23.3 years) were scanned on a 7-T MRI system (Magnetom Terra, Siemens Healthineers) under an IRB approved protocol. Images were acquired using a 1Tx/32Rx coil array and a 2D-EPI sequence with an unbalanced PCASL preparation pulse train. The vendor supplied ‘brain’ automatic shimming (up to second order) was performed at the beginning of each experiment with a shim region covering the brain and the tagging location (bottom of the cerebellum). The PCASL parameters were: selection gradient (Gmax)=3.5mT/m, mean gradient (Gmean)=0.25mT/m, Hanning RF pulse duration/separation=800/1700$$$\mu$$$s, B1 peak amplitude=5.7$$$\mu$$$T, labeling duration (LD)=1.5s and post-labeling delay (PLD) =1.5s. These parameters were chosen to minimize the time between the PCASL RF pulses while not exceeding the SAR limits. The 2D-EPI parameters were: matrix=64x64, resolution=3x3x3mm3, slices=23, TE/TR=12/4500ms, Grappa factor=2 and TA=6min.Four PCASL acquisitions were performed using different off-resonance compensation strategies: (i) no correction, (ii) prescan based correction (PScor), (iii) field-map based correction (FMcor), and (iv) average correction (AVGcor). PCASL prescan data were acquired using a balanced PCASL scheme with a LD/PLD 1000/300ms and tagging RF phase increments ranging from -180 to 180 deg with 22.5 deg increments.The field map at the tagging plane was acquired using a FLASH sequence (resolution=2.5x2.5x2.5mm3, TR=25ms, TE=1.8ms). A 1x1x1mm3 time-of-flight angiogram was acquired at the tagging plane to localize the feeding arteries.
The prescan and the field map data were processed offline using Matlab. In PScor, the PCASL inter-pulse phase angle error ($$$\triangle\phi$$$) was deduced from a cosine fit to the prescan data for the three main perfusion territories. In FMcor, the phase angle error was determined by $$$\triangle\phi$$$ = $$$2\pi\triangle$$$B0 $$$\triangle t \left(1-\frac{Gmean}{Gmax}\right)$$$ where $$$\triangle$$$B0 is the vessel specific field offset around the right internal carotid, the left internal carotid and between the two vertebral arteries. $$$\triangle t$$$ is the PCASL RF pulse separation. The $$$\triangle\phi$$$ values of each method were used to calculate the optimum PCASL correction parameters as described previously6. For AVGcor, the average of the field offsets around the feeding arteries was used to calculate a PCASL RF phase increment directly. In each data set, the normalized perfusion signal ((control-tag)/M0) was quantified in the three perfusion territories using manually drawn regions of interest in the four central slices.
Results
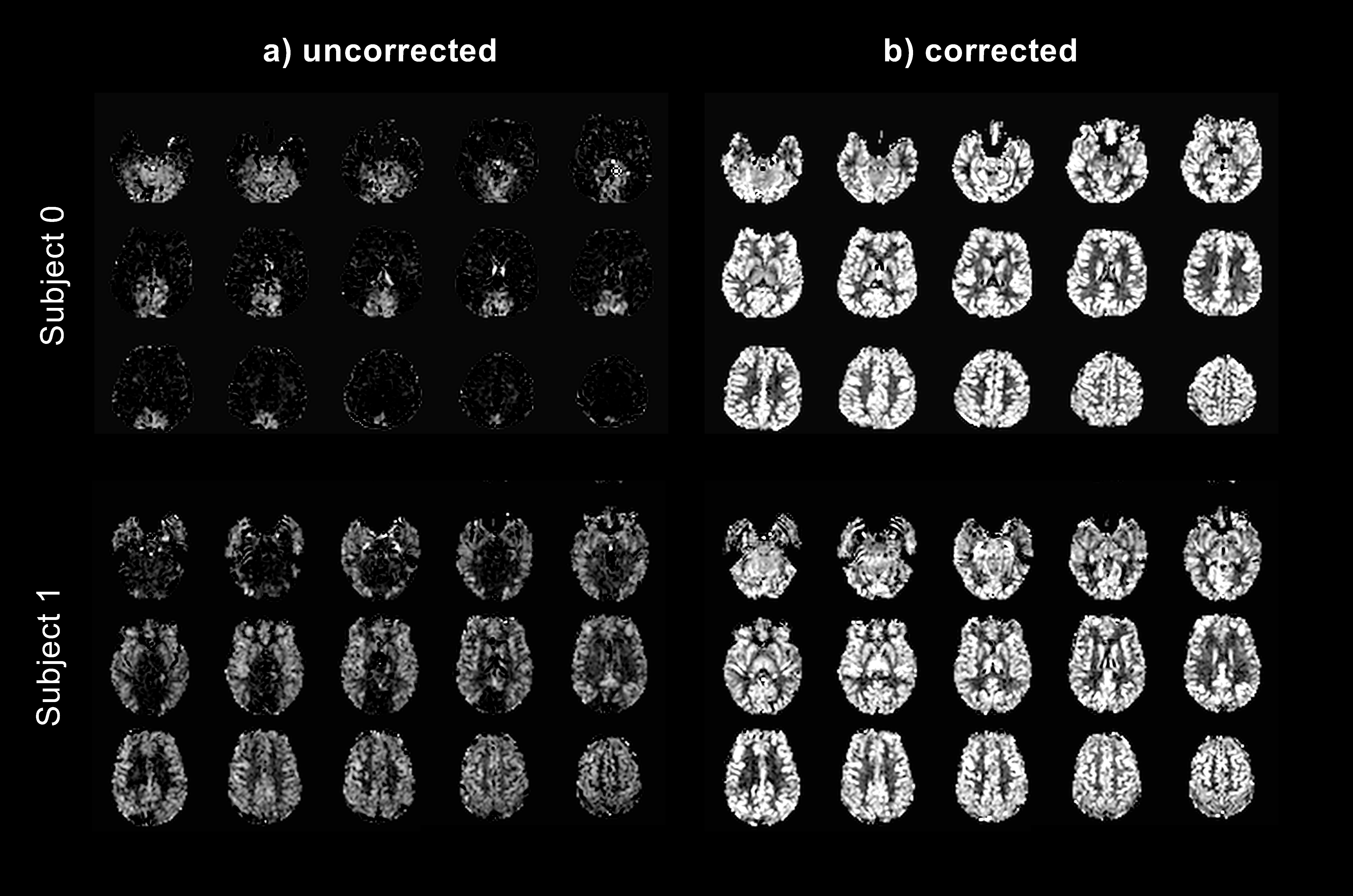
Table 1 presents the phase angle error $$$\triangle\phi$$$ determined from prescan and field map data. This shows a large inter-subject variability with an average $$$\triangle\phi$$$ of -82$$$\pm$$$33deg. Figure 1 shows perfusion data obtained from 2 subjects without and with off-resonance correction using FMcor. In data acquired without correction, the perfusion signal is observed in either the posterior or the anterior territory only (Fig. 1a). However, with FMcor, the perfusion signal is observed uniformly thoughout the brain (Fig. 1b). The normalized perfusion signal measured for all data sets is shown in Figure 2. On average, the perfusion signal increased by a factor of 2.6, 2.9 and 2.7 after PScor, FMcor and AVGcor, respectively.Discussion
This work shows that subject specific PCASL off-resonance compensation is necessary to acquire good quality cerebral perfusion images at 7T. The large inter-subject variability of the off-resonance field leads to highly variable image quality and reduced perfusion without off-resonance correction. In this study, all three correction methods vastly improved the perfusion signal in all the territories leading to uniform perfusion throughout the brain. FMcor and AVGcor performance was similar and slightly better than PScor, but these trends need to be confirmed with a larger subject population. Further improvement of PCASL at 7T may be possible by incorporation of off-resonance gradient corrections8.Acknowledgements
No acknowledgement found.References
1. Alsop DC, Detre JA, Golay X et. al., Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn. Reson. Med. 2015;73(1):102-16.
2. Jung Y, Wong E, Liu T, Multiphase Pseudocontinuous arterial spin labeling (MP-PCASL) for robust quantification of cerebral blood flow. Magn. Reson. Med. 2010;64:799-810.
3. Shin D, Liu T, Wong E, Shankaranarayanan A et. al., Pseudocontinuous arterial spin labeling with optimized tagging efficiency. Magn. Reson. Med. 2012;68:1135-1144.
4. Zhao L, Vidorreta M, Soman S et. al., Improving the robustness of pseudo-continuous arterial spin labeling to off-resonance and pulsatile flow velocity. Magn. Reson. Med. 2017;78:1342-1351.
5. Boland M, Stirnberg R, Pracht E et al., Robust and SAR-efficient whole-brain pseudo-continuous ASL at 7T. Proceedings ISMRM 2019; 4963.
6. Luh WM, Talagala SL, Li TQ et. al., Pseudo-continuous arterial spin labeling at 7T for human brain: estimation and correction for off-resonance effects using a prescan. Magn. Reson. Med. 2013;69:402-410.
7. Hirschler L, Debacker CS, Voiron J et al., Interpulse phase corrections for unbalanced pseudo-continuous arterial spin labeling at high magnetic field. Magn. Reson. Med. 2018;79:1314-1324.
8. Jahanian H, Noll DC, Hernandez-Garcia L, B0 field inhomogeneity considerations in pseudo-continuous arterial spin labeling (pCASL): effects on tagging efficiency and correction strategy. NMR BioMed. 2011;24,1202-1209.
9. Berry E, Jezzard P, Okell T, Off-resonance correction for pseudo-continuous arterial spin labeling using the optimized encoding scheme. NeuroImage 2019; 199:304-312.
Figures