When Will Non-k-Space-Based MRI Become a Clinical Reality?
1Mayo Clinic, United States
Synopsis
The purpose of this presentation is to describe the various levels of efficacy or value which are faced by a new technique which is being considered for clinical implementation, including the motivation for these. Further, this general framework is expanded upon for techniques which might be considered “non-traditional.”
Target Audience:
MRI researchers and clinicians interested in the technical-to-clinical evolution of new encoding techniquesOutcome:
The attendee will ideally be able to appreciate some of the issues and considerations in converting a new MRI technique into clinical usage as well as how these can be more stringent for non-traditional methods.Purpose:
The purpose of this presentation is to describe the various levels of efficacy or value which are faced by a new technique which is being considered for clinical implementation, including the motivation for these. Further, this general framework is expanded upon for techniques which might be considered “non-traditional.”Introduction:
Although MRI has been used for routine clinical application since the early 1980s, it has been under continuous technical development ever since its origins. Some developments are major or transformational, others less so. However, every year enhancements to commercial systems are provided which are then used routinely for clinical work. In considering whether some group of new methods such as “non-k-space-based MRI” becomes a clinical reality, it is useful to review the context of how new methods do eventually become “clinical.” In this presentation we review the general framework for consideration of new imaging techniques and as part of this consider the specific field, MRI, within which this is done.Background:
At the outset it is useful to note several aspects about the field, MRI, within which we work. When commercialization of MRI systems began in the early-to-mid 1980s, to their credit industrial vendors recognized that the field of MRI was so broad and fertile for study they could not investigate the many opportunities for study solely by themselves. This led to a concerted effort to foster research collaboration. However, rather than being a traditional collaboration in which a clinical group was asked to evaluate in patients some new, vendor-provided software “package,” this rather was a collaboration in which vendors expected their academic partners to investigate some technical problem or question. Moreover, vendors typically provided and even created the tools to perform these investigations on the vendor’s MRI equipment. This environment is far more amenable to academic development of new techniques than, say, the companion field of computed tomography (CT). That is to say, MRI is a field in which commercialization of developments of academic research, i.e. conversion of a new technique into clinical use, has been well recognized by MRI vendors.
The field abounds with examples of academically-developed techniques having been converted to clinical use. Very early examples include the encoding of multiple k-space lines per repetition interval in non-EPI sequences, incorporation of additional RF or gradient pulses to reduce artifact, and non-sequential ordering of phase encodings. More recently, acceleration techniques and statistical means for reconstruction have been commercialized and are used clinically. In virtually all of these cases some generally accepted premise or assumption of MR image formation was shown by the new development to be unnecessarily and disadvantageously limiting.
Value:
Expansion or extension of a new research technique into broader clinical use depends fundamentally on the value of the technique in the eyes of the would-be user group. For clinical use of MRI, the user group is comprised of the owners or overseers of the MRI scanners. Methods which allow more efficient or expanded use of the MRI scanner can potentially add value.
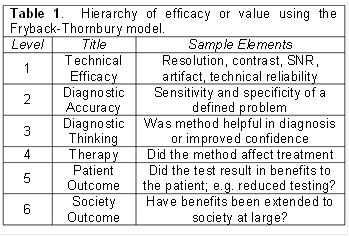
It is important to recognize that the value of some new technique, such as a specific MRI acquisition method, call it Test X, can be considered using a hierarchical model. At progressively higher levels in the hierarchy the technique has expanded value. One such model for medical imaging is that of Fryback and Thornbury [1] which was first proposed in the early 1990s. Analogous hierarchies have been developed and are used in assessing other forms of biomedical technology, such as the Technology Readiness Level (TRL) by DOD. The Fryback-Thornbury hierarchy is shown in abbreviated form in Table 1. The lowest level is that of technical efficacy. This includes not only demonstration of adequate performance of the relevant physical quantities such as resolution and contrast, but also a presumed very high level of technical reliability. The next level of efficacy indicated is that of diagnostic accuracy. How well does the new method perform in the sensitivity and specificity for a particular medical test? The next level deals with how the new technique may impact diagnostic thinking. At this level one assesses what the potential impact of Test X might be vis-à-vis other data available to the clinician, such as laboratory data or results from other imaging tests, both MRI and non-MRI. As seen, the hierarchy continues, culminating in consideration of the value or efficacy at a societal level.
Of course, it is unreasonable to expect that the developers of Text X will evaluate their new method at all levels. In fact, it is undesirable that this be done because of questions of bias. However, it is important that the developers understand that a hierarchy of efficacy and value exists. At the lowest level the developers of Test X or their collaborators should identity the relevant technical criteria which the technique must meet and show that Test X can be successfully performed in some representative group of subjects. At Level 2, are there specific diagnostic tests or conditions which might conceivably be performed with Test X? At Level 3, might the results of Text X somehow be used in the decision-making of the clinician? For the case of accelerated scans or abbreviated protocols, can truly equivalent diagnostic performance be provided with a substantial reduction in exam time and improvement in workflow?
Prospects for Non-k-Space-Based MRI:
The need for establishment of value of some new technique and the presumed, associated clinical implementation may appear daunting. However, at some level virtually all techniques currently offered as part of MRI systems are there because they were seen as having some value after being subjected to some form of the above hierarchy of assessment.
Technique developers who strive for their methods to become “clinical” and MRI manufacturers have congruent interests. If Test X can be shown to have clinical value, then it is in manufacturers’ interests to make that test available in their products and sell it to the MRI user base.
At the end of the 20th Century there were many polls made and lists generated of the most influential people, events, literary and artistic works of the previous century. In this spirit a survey of several hundred medical practitioners, all general internists, was made asking them to rank which of several dozen developments of the previous 25 years was most influential in their practice [2]. These developments included various new drugs, blood tests, surgical procedures, and other methods. Ranked at the very top of the list by a sizeable margin was the combination of MRI and CT scanning. That is to say, the medical community found great value in these imaging methods. Interestingly, looking back at the past 20 or so years, there are multiple additional enhancements to MRI systems which were not widely available clinically at the time the survey was done but which are now commonplace today. These include various acceleration techniques and diffusion-weighted imaging to name two. In addition, MRI today is seeing considerably expanded use in areas not widely studied in 2000. Examples include the imaging of prostate cancer and in radiation therapy treatment planning. MRI in general is seen by the medical community as having high value, and its impact continues to expand.
To summarize, the path to clinical reality of contemporary research developments is similar to that followed of previous innovations which are now clinical. It is incumbent on the proponents of a new technique to, if not demonstrate, then show the high likelihood of value of their method.
Acknowledgements
No acknowledgement found.References
[1] Thornbury JR. Clinical efficacy of diagnostic imaging: love it or leave it. Amer J Roentgenol 1994;162:1-8.
[2] Fuchs VR, Sox HC. Physicians' views of the relative importance of thirty medical innovations. Health Affairs 2001;20:30-42.
Figures