2040
Simultaneous High-resolution 3D Whole-heart Bright-Blood Coronary Angiography and Black-Blood Late Gadolinium Enhancement (LGE)1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
The T2-prepared BOOST sequence was recently introduced for simultaneous post-contrast 3D whole-heart bright-blood coronary angiography and black-blood late gadolinium enhancement (LGE) imaging. This sequence enables simultaneous visualization of cardiac anatomy, the coronary arteries and scar tissue. However, high-resolution fully-sampled BOOST requires long acquisition times of ~20min. Here, we propose to accelerate the T2-prepared BOOST sequence and achieve high spatial resolution 3D whole-heart black-blood LGE and coronary MR angiography. This is accomplished by extending XD-ORCCA, a highly efficient respiratory-resolved motion-corrected framework, to BOOST imaging. The proposed framework enables simultaneous black-blood LGE and bright-blood coronary angiography within clinically feasible acquisition times.
Introduction
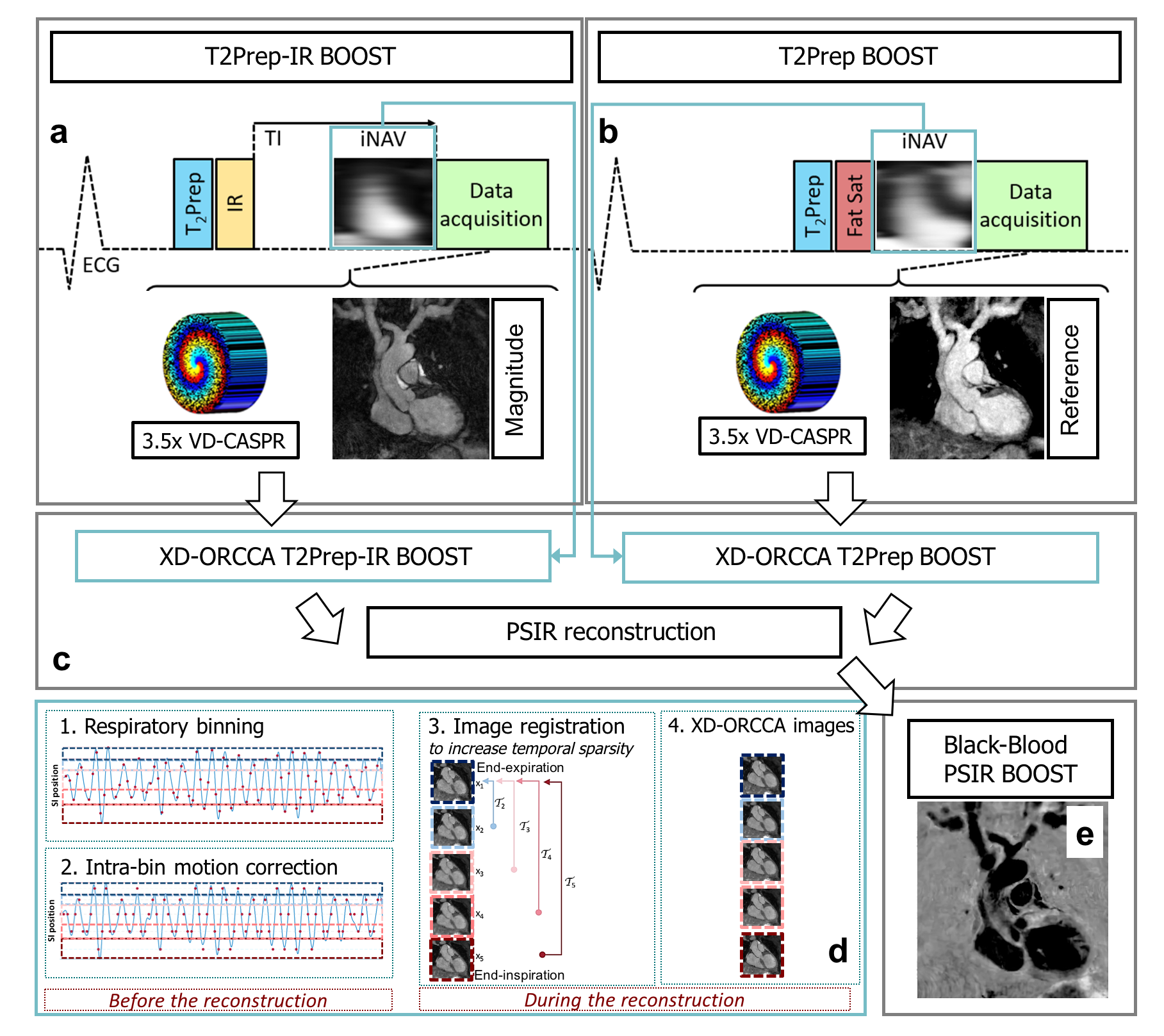
Phase sensitive inversion recovery (PSIR) reconstruction applied to late gadolinium enhancement (LGE) imaging is widely used for detecting myocardial infarction.1 However, conventional 2D PSIR LGE provides limited coverage of the heart and acquisitions are performed under breath-hold. Recently, the free-breathing T2-prepared BOOST sequence was proposed for simultaneous 3D whole-heart bright-blood coronary angiography and black-blood LGE.2 This sequence allows for LGE visualization with improved volumetric coverage and contrast with respect to the contiguous blood-pool. Moreover, it provides a complementary bright-blood volume for cardiac anatomy and coronary lumen visualization. However, high-resolution BOOST requires long acquisition times of ~20min. Here, we propose to accelerate T2-prepared BOOST to enable high-resolution whole-heart coronary MR angiography and black-blood LGE in a more clinically feasible timeframe of <10min. This is achieved by extending a robust and highly efficient respiratory-resolved motion-compensated framework (XD-ORCCA) that was originally introduced for fully-sampled 3D Cartesian images.3 This method uses 2D translational motion information extracted from image navigators (iNAVs)4 to increase the sparsity in the respiratory dimension and to compensate for residual motion within each respiratory bin (Fig.1). The proposed method was tested in five patients with cardiovascular disease.Methods
Accelerated 3D T2-prepared BOOST uses a variable-density Cartesian trajectory with spiral profile order (VD-CASPR).5,6 The BOOST sequence alternates the acquisition of a T2-prepared Inversion Recovery module (T2Prep-IR, odd heartbeats) and a T2-prepared module (T2Prep, even heartbeats) (Fig.1). Low-resolution 2D iNAVs are acquired at every heartbeat and used to estimate beat-to-beat 2D translational motion and obtain the respiratory signal, which is used to distribute each BOOST dataset into five equally populated respiratory bins. Respiratory-resolved images $$$\mathbf{x}$$$ for each BOOST dataset are obtained by solving a modified version of XD-ORCCA: $$$\hat{\mathbf{x}}=\arg\min\limits_{\mathbf{x}}\left\{\frac{1}{2}\left\|\mathbf{E}\mathbf{x}-\mathbf{d}\right\|^2_2+\alpha\,\Psi_{\textrm{t}}\left(\mathcal{R}\mathbf{x}\right)+\beta \,\Psi_{\textrm{-t}}\left(\mathcal{R}\mathbf{x}\right)+\gamma \,\Psi_{\textrm{s}}\left(\mathbf{x}\right) \right\}$$$, where $$$\mathbf{d}$$$ are the 2D intra-bin translational motion-corrected k-space data, $$$\Psi_{\textrm{s}}$$$ is the 3D spatial total variation (TV) function, $$$\alpha$$$, $$$\beta$$$ and $$$\gamma$$$ are regularization parameters, $$$\mathcal{R}\mathbf{x}=\mathcal{T}_b\mathbf{x}_b$$$ is the translational motion-corrected domain, where $$$\mathcal{T}_b$$$ is the translation transform that maps the respiratory bin image $$$\mathbf{x}_b$$$ to the reference image $$$\mathbf{x}_1$$$ (end-expiration), $$$\Psi_{\textrm{t}}=\left\| \mathcal{T}_b\mathbf{x}_b - \mathcal{T}_{b+1}\mathbf{x}_{b+1}\right\|_1$$$ and $$$\Psi_{\textrm{-t}}=\left\| \mathcal{T}_b\mathbf{x}_b -\mathcal{T}_{b-1}\mathbf{x}_{b-1}\right\|_1$$$ are 1D temporal TV functions. The operator $$$\mathbf{E}=\mathbf{A}_b\mathbf{FS}$$$ incorporates the sampling matrix $$$\mathbf{A}_b$$$ for each bin $$$b$$$, Fourier transform $$$\mathbf{F}$$$ and coils sensitivities $$$\mathbf{S}$$$. Finally, the T2Prep-IR and T2Prep BOOST images are combined in a PSIR-like reconstruction.
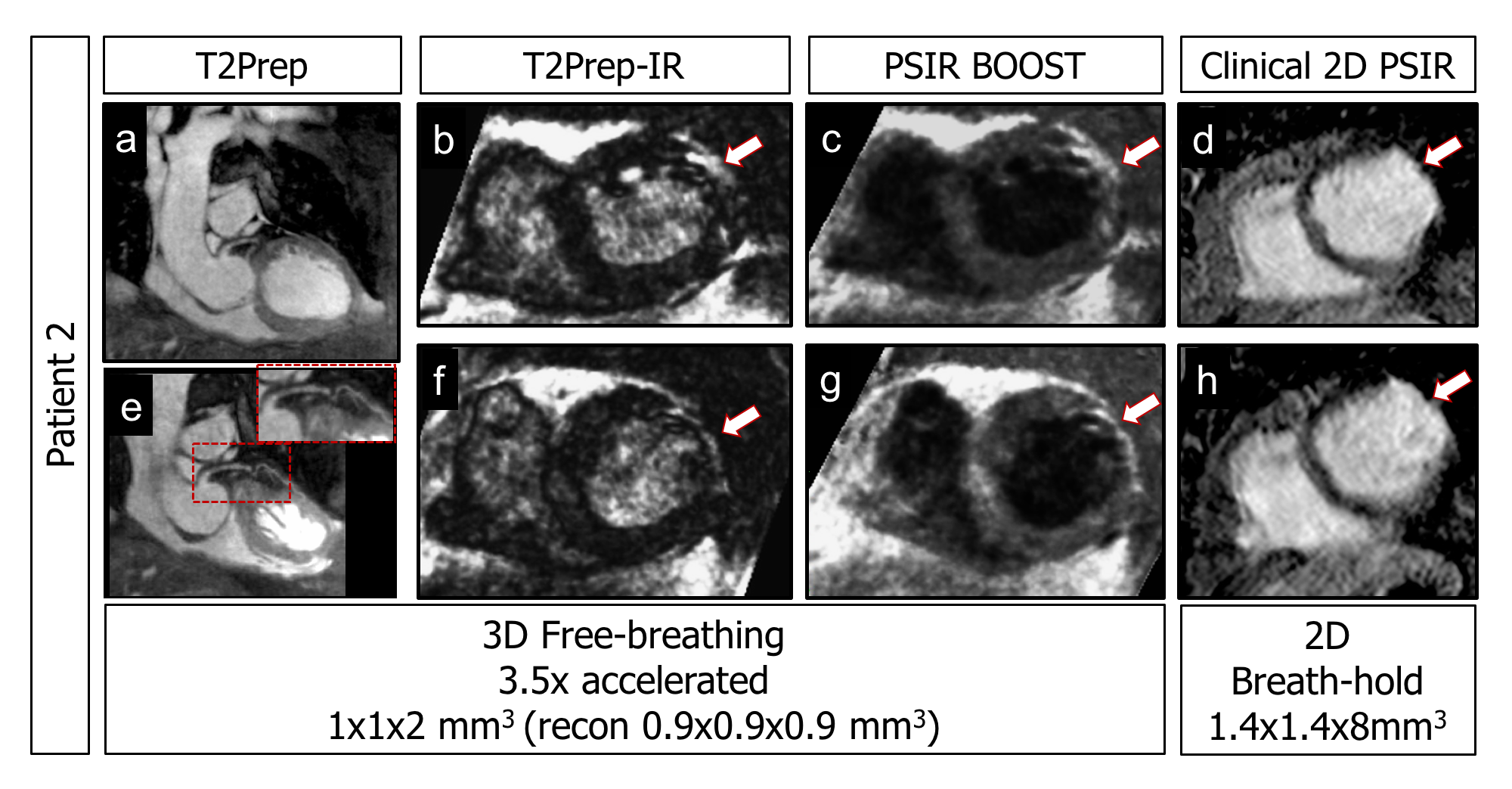
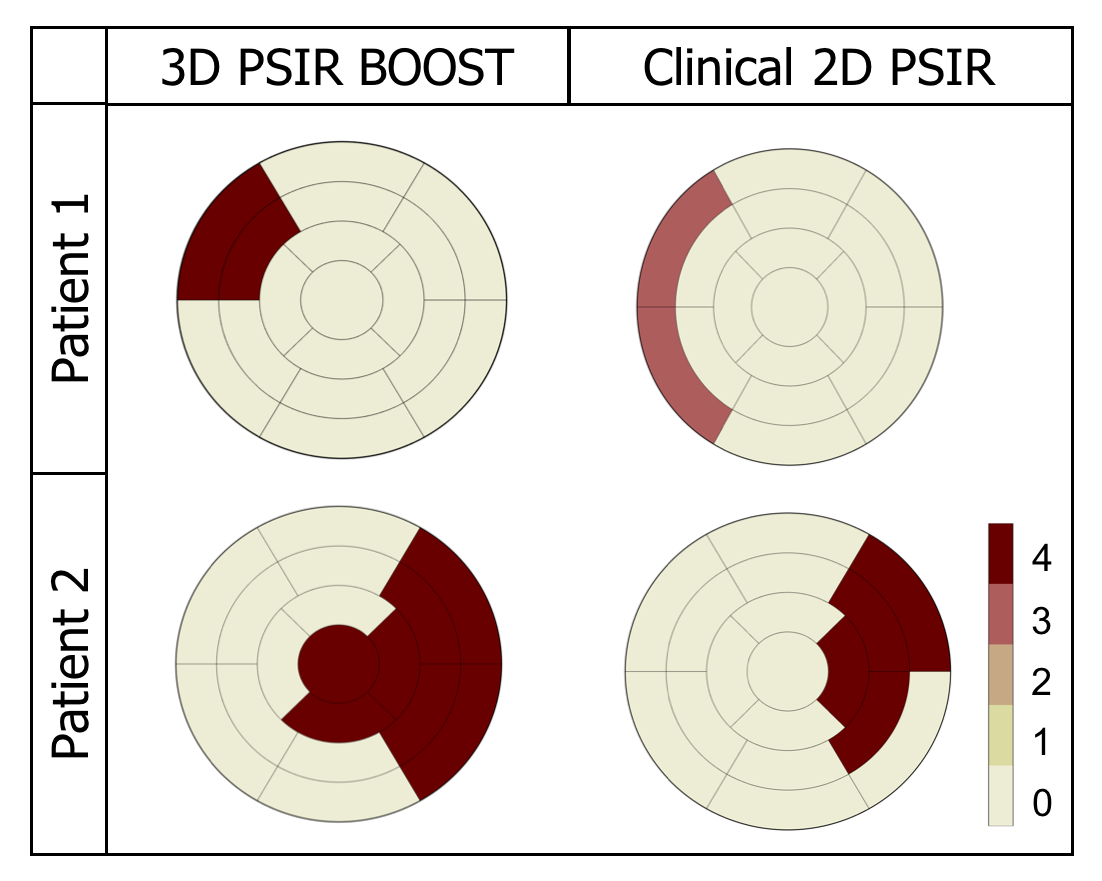
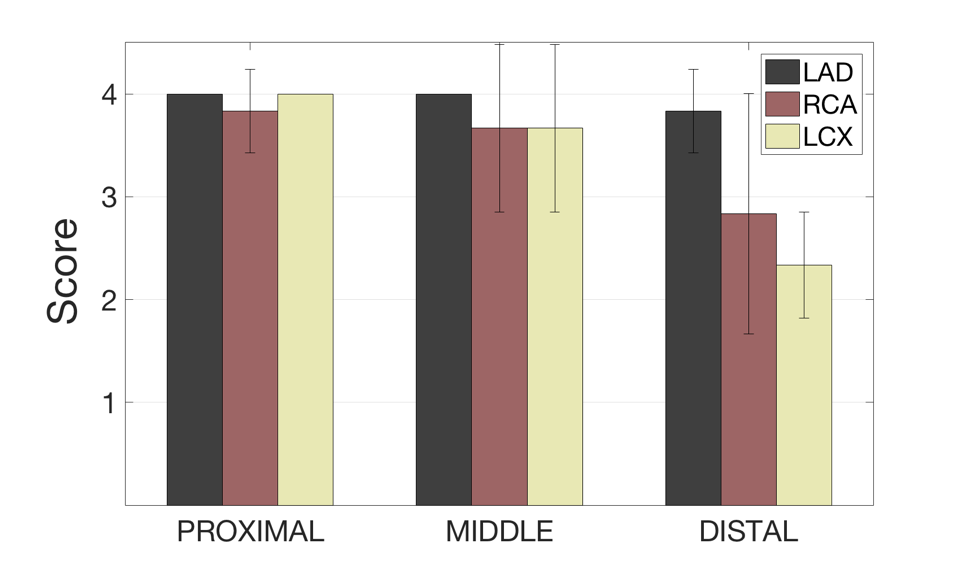
Free-breathing acquisitions were performed in five patients with cardiovascular disease on a 1.5T scanner (Siemens Magnetom Aera). A multi-slice and multi breath-hold 2D-PSIR LGE clinical sequence was acquired ~8min after Gadobutrol injection (0.2mmol/kg) with a spatial resolution of 1.4x1.4x8mm3. Subsequently, BOOST acquisitions were performed (~20-25min after injection) using the following parameters: coronal orientation, FOV=320x320x96-128mm3, resolution=1x1x2mm3 (reconstructed to 0.9x0.9x0.9mm3), TR/TE=3.6/1.56ms, flip-angle=90°, subject-specific TI=90-250ms, T2Prep=40ms, 3.5-fold undersampling and acquisition time 7min11s±50s. Blinded qualitative grading of anonymized clinical 2D PSIR and 3D PSIR BOOST images was performed by two cardiologists (SCMR III accredited). The transmural extent of LGE was graded using a 17-segment model and 5-point scale: 0) none, 1) 1-25%, 2) 26-50%, 3) 51-75%, 4) 76-100%. Moreover, the diagnostic quality of the proximal, mid and distal sections of the left anterior descending coronary artery (LAD), left circumflex coronary artery (LCX), and right coronary artery (RCA) course, was graded using a 4-point scale: 1) non-diagnostic, 2) diagnostic with major artifacts, 3) diagnostic with minor artifacts and 4) fully diagnostic.
Results
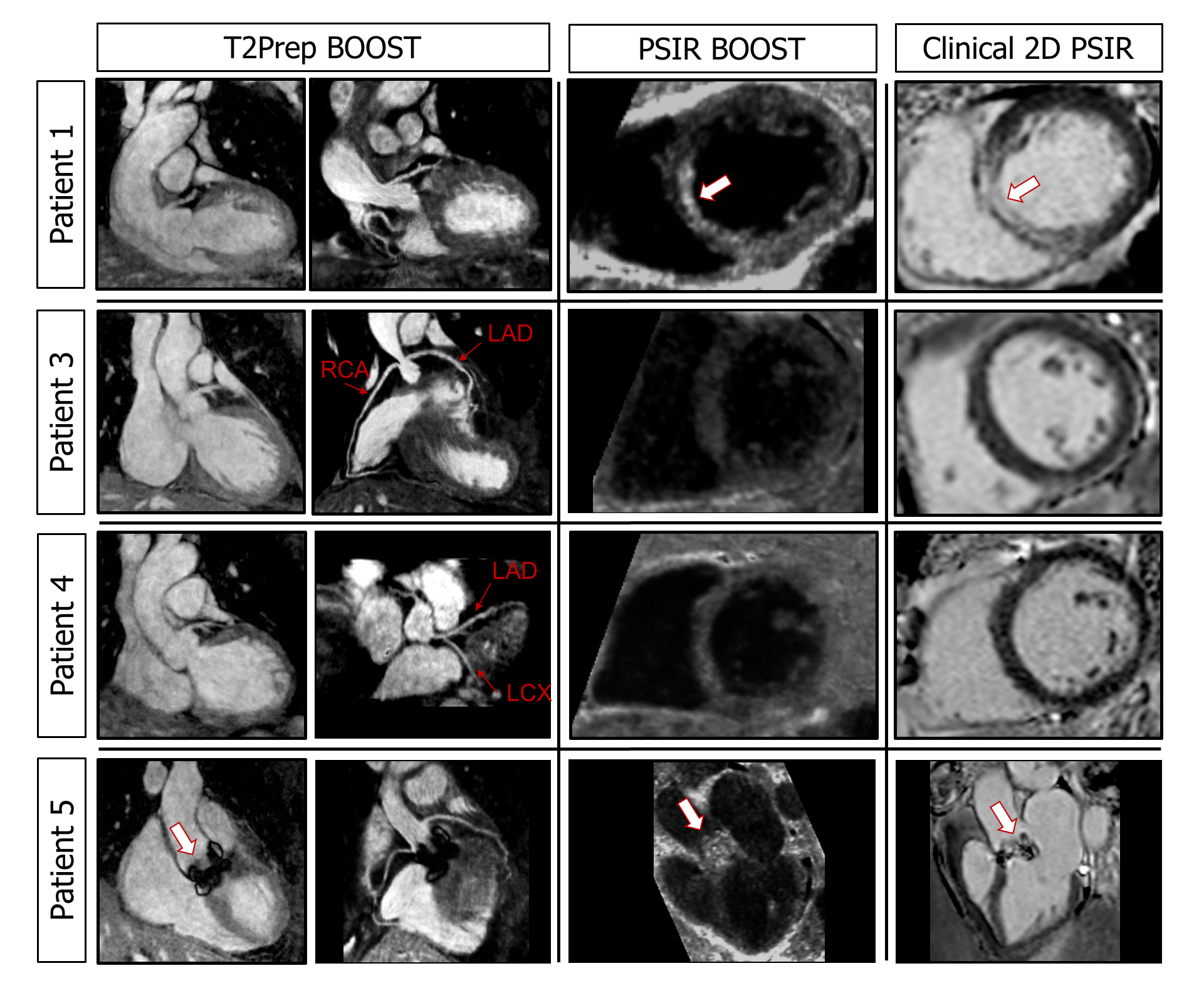
The clinical 2D PSIR and proposed 3D BOOST images (T2Prep, T2Prep-IR and PSIR) are shown in Figure 2 for a patient with ischemic cardiomyopathy. For all patients, the regions of LGE uptake on PSIR BOOST images were in good agreement with clinical 2D PSIR images (Figs2-3) with visualization of scar (patient 1&2) despite image acquisition >20min after contrast administration. This was facilitated by the high contrast between scar tissue and blood pool in 3D PSIR BOOST images compared to clinical 2D PSIR. No significant differences (p>0.05) in transmurality were found between the 2D clinical PSIR and 3D BOOST PSIR. The 17-segment scores obtained for the clinical 2D and high-resolution 3D PSIR BOOST for two patients with ischemic scar are shown in Figure 4. 3D PSIR BOOST detected similar territories of LGE (myocardial infarction) compared with clinical 2D PSIR. Moreover, T2Prep BOOST allowed for visualization of proximal and middle LAD, LCX and RCA sections with high diagnostic quality (Fig.5).Conclusions
The proposed framework provides high‐resolution post-contrast 3D whole-heart bright-blood and black-blood LGE images in ~7min, allowing for visualization of scar tissue and cardiac anatomy from a single acquisition in a clinically feasible timeframe. This was achieved by combining XD-ORCCA respiratory-resolved reconstruction with 3D whole-heart Cartesian T2-prepared BOOST undersampled acquisitions.Acknowledgements
This work was supported by the following grants: EPSRC EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1 and Wellcome EPSRC Centre for Medical Engineering NS/A000049/1.References
1. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med 2002; 47:372-83.
2. Ginami G, Neji R, Rashid I, Chiribiri A, Tevfik I, Botnar RM, Prieto C. 3D whole-heart phase sensitive inversion recovery CMR for simultaneous black-blood late gadolinium enhancement and bright-blood coronary CMR angiography. J Cardiovasc Magn Reson 2017; 19:94.
3. Correia T, Ginami G, Cruz G, Neji R, Rashid R, Botnar RM, Prieto C. Optimized respiratory‐resolved motion‐compensated 3D Cartesian coronary MR angiography. Magn Reson Med 2018; 80:2618-2629.
4. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med 2012; 67:437-445.
5. Correia T, Cruz G, Schneider T, Botnar RM, Prieto C. Accelerated nonrigid motion-compensated isotropic 3D coronary MR angiography. Med Phys 2018; 45:214-222.
6. Prieto C, Doneva M, Usman M, Henningsson M, Greil G, Schaeffter
T, Botnar RM. Highly
efficient respiratory motion compensated free-breathing coronary MRA using
golden-step Cartesian acquisition. J Magn
Reson Imaging 2015; 41:738-46.
Figures