2011
Myocardial T1 mapping using inversion recovery with radial simultaneous multi-slice readout and model-based reconstruction1UCAIR, University of Utah, Salt Lake City, UT, United States, 2Physics, University of Utah, Salt Lake City, UT, United States
Synopsis
Here we propose an inversion recovery based radial simultaneous multi-slice sequence for myocardial T1 mapping. 3 slices of T1 maps were acquired simultaneously within one breath hold spanning 11 heartbeats. Model based reconstruction was used to jointly reconstruct images at different inversion times and estimate T1 maps. Native T1, post-contrast T1 and ECV maps agree with results from the slice-by-slice Cartesian MOLLI sequence.
Introduction
Myocardial T1 mapping is an important clinical tool that can discriminate multiple cardiac diseases. The standard slice-by-slice methods require multiple breath-holds to acquire whole heart T1 maps. Several approaches have been studied to increase the acquisition efficiency by using 3D saturation recovery (SR) base sequences (1,2), or SR based Cartesian simultaneous multi-slice (SMS) techniques (3). Radial non-SMS inversion recovery (IR) based sequences have also been proposed to accelerate T1 acquisitions (4-6). Here we improve our work that used a single shot IR to acquire 3 slices of myocardial T1 maps (7) by using two IR pulses within a breath hold and measurements at 8 inversion times (TIs). For the reconstruction, we included a model based regularization within a compressed sensing framework to jointly reconstruct images at different TIs while concurrently estimating T1 maps. Pre- and post-contrast T1 maps were acquired using the proposed method and ECV maps were calculated. The results were compared with a Cartesian MOLLI sequence.Method
Sequence
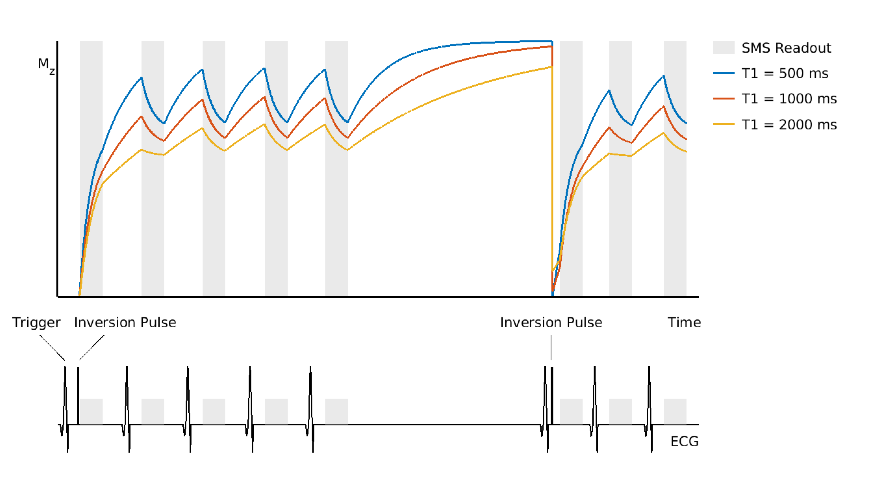
A nonselective 180o pulse (6-pulse train (8)) was applied after receiving an ECG trigger and the trigger delay time was set to receive data during the diastolic phase. 150 radial k-space rays were acquired with a golden-angle sampling pattern, and five such readouts were done in 5 heartbeats. After recovery for 3 heartbeats, another IR was applied and 3 more 150-ray-readout were acquired. The first readout started ~11ms after the first IR pulse and the sixth readout started ~100ms after the second IR (Figure 1). Three slices were read out simultaneously with a controlled aliasing (CAIPI) phase modulation pattern (9). The scan was done on a 3T Siemens (Prisma) scanner with breath hold with parameters: TR/TE 2.1/1.1ms, FOV 260mm2, flip angle 8o, voxel size 1.8x1.8x8mm3. Figure 1 illustrates the proposed pulse sequence.
Reconstruction
Model based reconstruction was built into the spatiotemporal constrained reconstruction (STCR) framework (10) to jointly reconstruct images and T1 maps. The cost function (1) was minimized:
$$m=\mathrm{arg min} \left( \left|\left|Am-d \right|\right|_2^2 +\lambda_s\left|\left|\sqrt{\nabla_xm^2+\nabla_ym^2+\epsilon}\right|\right|_1+\lambda_m\left|\left|m-\hat{m}_{\mathrm{mb}}\right|\right|_2^2\right). (1)$$
In addition to the data fidelity and spatial total variation terms as described in (10), the term $$$\lambda_m \left|\left| m - \hat{m}_{\mathrm{mb}}\right|\right|_2^2$$$ is an $$$l_2$$$ norm constraint of the difference between estimated image set and the model based image estimation $$$\hat{m}_{\mathrm{mb}}$$$. $$$\hat{m}_{\mathrm{mb}}$$$ is updated at every iteration by fitting T1 maps from $$$m$$$ using Bloch simulation and reproducing the model images at different TIs from the estimated T1 maps. Magnitude values of $$$m$$$ were used for the T1 fitting, the phase of $$$\hat{m}_{\mathrm{mb}}$$$ was kept the same as $$$m$$$. The T1 fitting used a pattern recognition algorithm from (6) with a dictionary of 5 flip angle variations (0.6-1 of the value set on the scanner) and 2701 T1 values (300-3000ms) for native T1, and 2000 T1 values (1-2000ms) for post-contrast T1. The radial SMS data was interpolated onto a Cartesian grid before iterative reconstruction using an SMS GROG method (11). To improve image quality, the k-space of measurement 1 included additional k-space rays from measurement 6 though using only the high frequency part of the rays. This was done in the same way for measurements 2-3 with 7-8 and vice versa.
Result
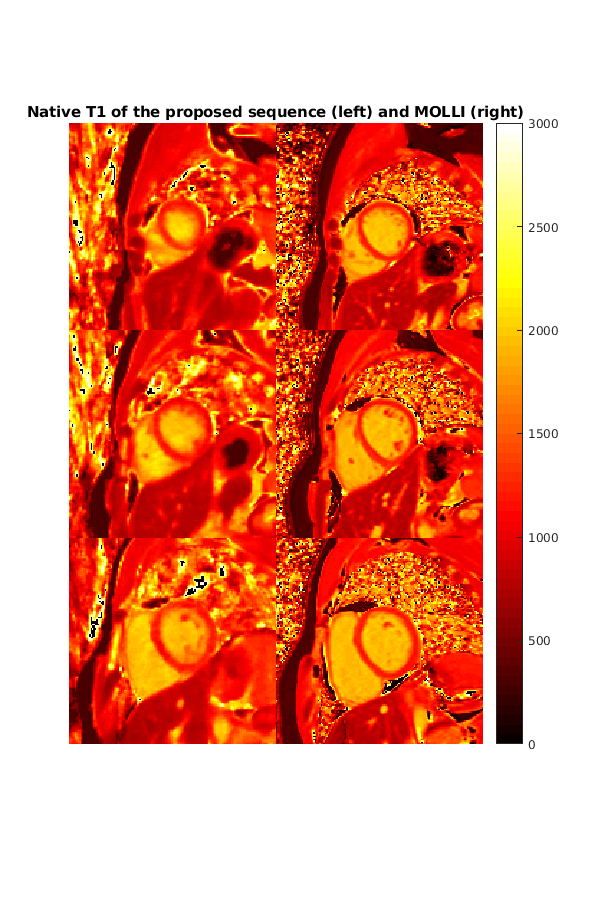
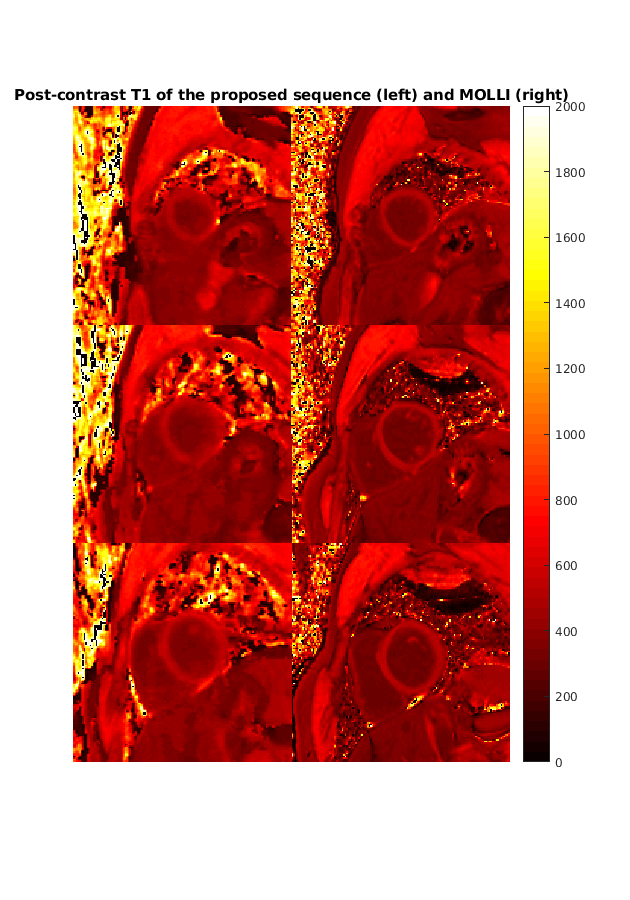
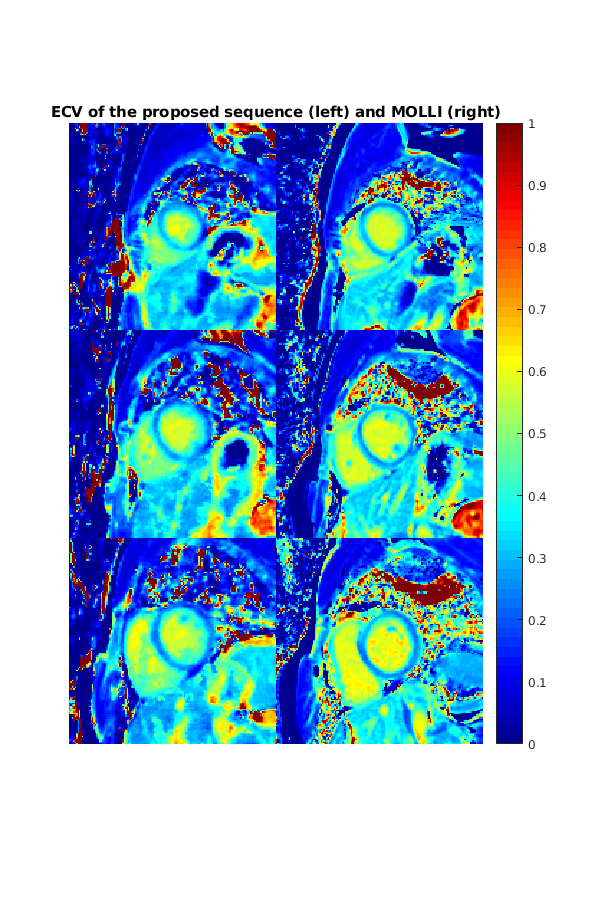
Figure 2 shows the reconstructed images at different TIs. Corresponding native T1 maps are shown in Figure 3. T1 maps acquired using a slice-by-slice Cartesian MOLLI sequence are also shown. Figure 4 compares the post-contrast T1 maps with the Cartesian MOLLI sequence. The mean native myocardial T1 value computed from all the three slices was 1201.6 ± 87.0 ms (proposed sequence) and 1211.0 ± 63.8 ms (MOLLI), and the mean post-contrast T1 was 492.6 ± 77.9 ms (proposed sequence) and 506.6 ± 24.6 ms (MOLLI). The ECV maps calculated form the native and post-contrast T1 maps are shown in Figure 5. The ECV value was 26.5 ± 4.8 %, which agrees with the MOLLI result 26.6 ± 2.7 % and literature values (12).Discussion and Conclusion
Although not shown here we tested an interleaved slice-group radial SMS sequence to acquire 6 slices of T1 maps within one breath hold. Increased inconsistency of data due to a longer TR and higher undersampling rate degraded image quality.
The proposed IR radial SMS sequence was able to acquire 3 slices of myocardial T1 maps simultaneously for both pre- and post-contrast. By using the model based STCR reconstruction framework, 3 slices of T1 maps can be directedly reconstructed from the acquired radial SMS data. The native and post-contrast myocardium T1 and ECV values agree with the values from the Cartesian MOLLI sequence.
Acknowledgements
References
1. Nordio G, Henningsson M, Chiribiri A, Villa ADM, Schneider T, Botnar RM. 3D myocardial T1 mapping using saturation recovery. J Magn Reson Imaging 2017;46(1):218-227.
2. Nordio G, Bustin A, Henningsson M, Rashid I, Chiribiri A, Ismail T, Odille F, Prieto C, Botnar RM. 3D SASHA myocardial T1 mapping with high accuracy and improved precision. MAGMA 2018.
3. Weingartner S, Moeller S, Schmitter S, Auerbach E, Kellman P, Shenoy C, Akcakaya M. Simultaneous multislice imaging for native myocardial T1 mapping: Improved spatial coverage in a single breath-hold. Magn Reson Med 2017;78(2):462-471.
4. Wang X, Voit D, Roeloffs V, Uecker M, Frahm J. Fast Interleaved Multislice T1 Mapping: Model-Based Reconstruction of Single-Shot Inversion-Recovery Radial FLASH. Comput Math Methods Med 2018;2018:2560964.
5. Gensler D, Morchel P, Fidler F, Ritter O, Quick HH, Ladd ME, Bauer WR, Ertl G, Jakob PM, Nordbeck P. Myocardial T1: quantification by using an ECG-triggered radial single-shot inversion-recovery MR imaging sequence. Radiology 2015;274(3):879-887.
6. Marty B, Coppa B, Carlier PG. Fast, precise, and accurate myocardial T1 mapping using a radial MOLLI sequence with FLASH readout. Magn Reson Med 2018;79(3):1387-1398.
7. Ye Tian, Jason Mendes, Edward DiBella, Ganesh Adluru. Radial simultaneous multi-slice myocardial T1 mapping using single shot inversion recovery. 2019; Bellevue, WA USA.
8. Chow K, Kellman P, Spottiswoode BS, Nielles-Vallespin S, Arai AE, Salerno M, Thompson RB. Saturation pulse design for quantitative myocardial T1 mapping. J Cardiovasc Magn Reson 2015;17:84.
9. Yutzy SR, Seiberlich N, Duerk JL, Griswold MA. Improvements in multislice parallel imaging using radial CAIPIRINHA. Magn Reson Med 2011;65(6):1630-1637.
10. Adluru G, McGann C, Speier P, Kholmovski EG, Shaaban A, Dibella EV. Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging. J Magn Reson Imaging 2009;29(2):466-473.
11. Ye Tian, Ganesh Adluru, Jason Mendes, Edward Dibella. Evaluation of extended GROG and Toeplitz pre-interpolation methods on radial simultaneous multi slice MRI. 2018; Paris, France.
12. Dabir D, Child N, Kalra A, Rogers T, Gebker R, Jabbour A, Plein S, Yu CY, Otton J, Kidambi A, McDiarmid A, Broadbent D, Higgins DM, Schnackenburg B, Foote L, Cummins C, Nagel E, Puntmann VO. Reference values for healthy human myocardium using a T1 mapping methodology: results from the International T1 Multicenter cardiovascular magnetic resonance study. J Cardiovasc Magn Reson 2014;16:69.
Figures