0844
Optimization of time-encoded pseudo-continuous ASL angiography with a variable flip-angle scheme1Wellcome Center for Integrative Neuroimaging, University of Oxford, Oxford, United Kingdom, 2Insitute of Biomedical Engineering, University of Oxford, Oxford, United Kingdom
Synopsis
Time-encoded PCASL angiography is an attractive method for deriving some, or all, of the desired temporal information from the PCASL preparation rather than a dynamic readout. Higher flip-angles can then be used for the remaining excitation pulses in the readout, increasing the signal-to-noise ratio of the angiograms.
However, use of constant flip angles across all excitations leads to abrupt signal changes between images constructed from different time-encoding blocks. A variable flip-angle scheme is presented, which maintains a constant signal across all excitations, removes these discontinuities and ensures optimal signal levels across all images.
Introduction
Arterial spin labeling (ASL),1,2 where the magnetization of inflowing blood to the brain is inverted and used as an endogenous contrast agent, can be used to visualize blood flow through the arterial tree.3,4 Dynamic angiograms can be obtained by acquiring multiple sequential images after each ASL preparation using multiple excitation pulses.5,6 Since the ASL signal is attenuated by each excitation, low flip-angles are required, which limits SNR.
An alternative method for acquiring multiple time-points is to encode different post-labeling delays (PLDs) into a pseudo-continuous ASL (PCASL) preparation using a Hadamard encoding scheme,7 referred to as time-encoding. When the temporal information is obtained partly or entirely from the ASL preparation, rather than the readout, fewer excitations are required per ASL preparation and larger flip-angles can be used.8
Previous work demonstrated that a time-encoded preparation could preserve signal for more distal vessels.9 However, the use of a constant flip-angle (CFA) scheme results in greater signal attenuation at later time points within each block. This leads to abrupt signal changes between images constructed from different time-encoded blocks.
In this work, we use an optimal variable flip-angle (VFA) scheme to remove abrupt signal changes between time-encoded blocks and maximize the signal at later time points. We demonstrate the SNR advantage and improved distal vessel depiction with this approach compared to a matched sequential protocol, using simulations and in vivo experiments.
Methods
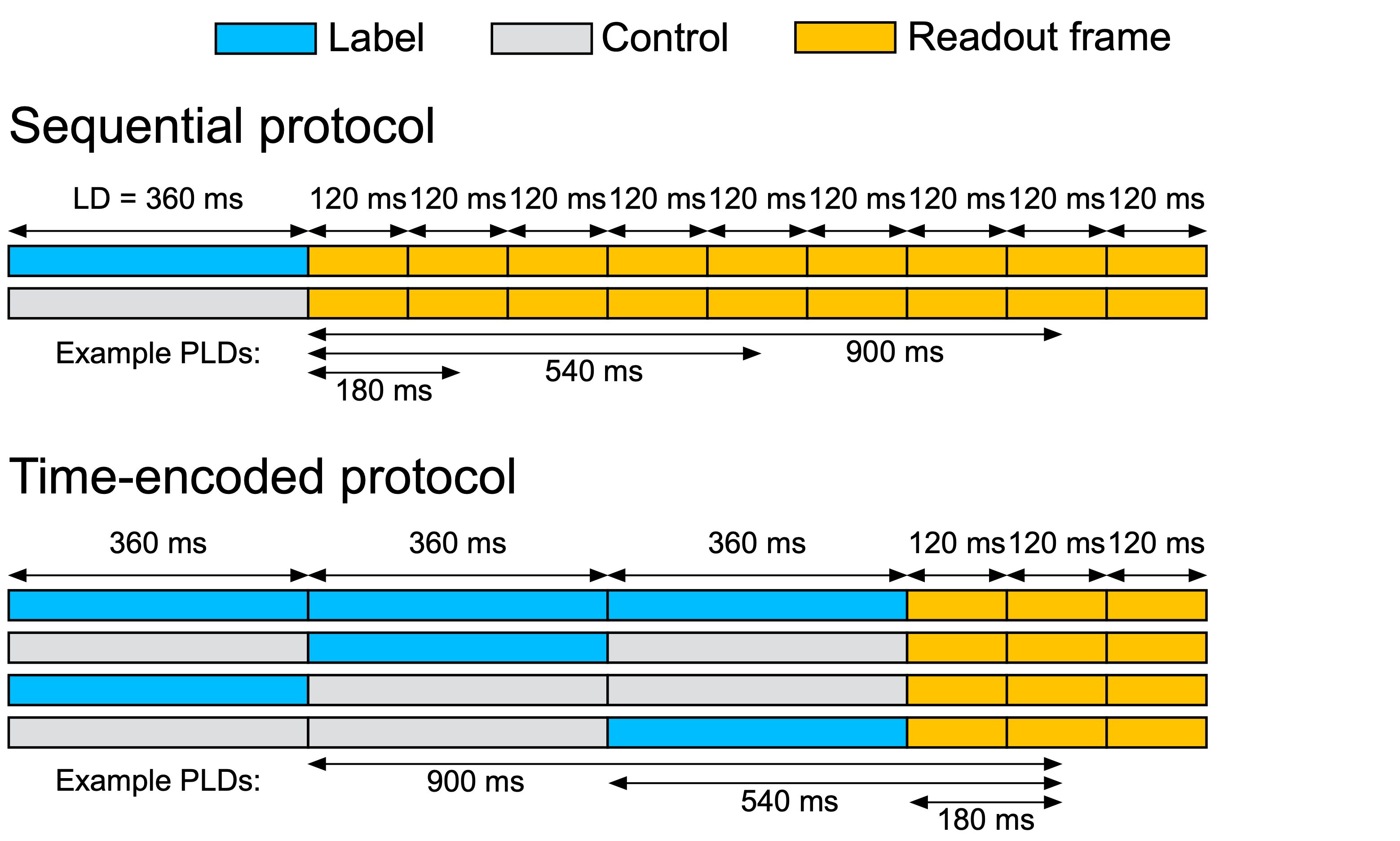
We compared a sequential PCASL protocol, with 9 temporal frames, to a 3-block time-encoded protocol, with 3 frames, giving matched label durations (LD): 360 ms and PLDs: 60, 180, 300, 420, 540, 660, 780, 900, 1020 ms (Figure 1).
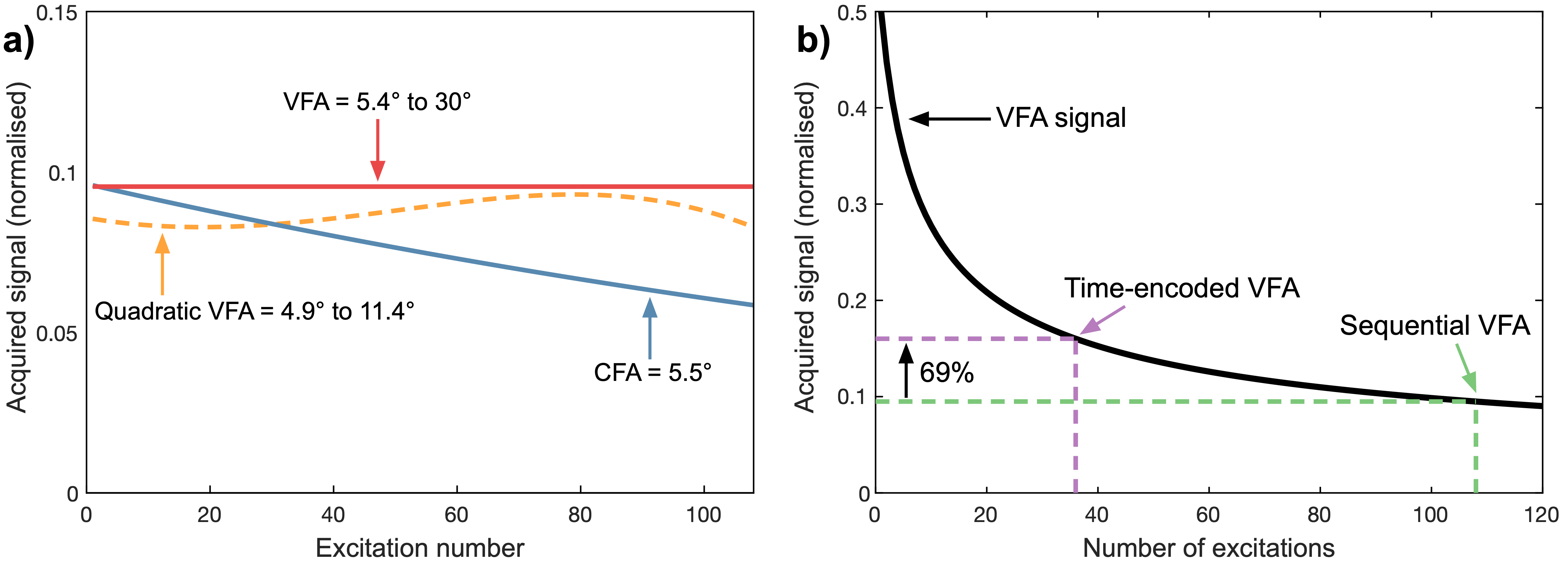
Both protocols were performed with two flip-angle schemes (Figure 2):
- A CFA scheme, optimized to maximize the acquired signal at the last excitation (sequential: 5.5°; time-encoded: 9.6°).
- A VFA scheme, which maintains a constant acquired signal of the ASL tracer in a given voxel (maintain VFA). This VFA scheme used a backwards recursive formula: θi-1=tan-1(sin(θi)), i=1,...,N, where θ is the flip angle. θN was set to 30°.
Simulations, using a previously proposed ASL angiography model,10 were used to compare the signal improvement for each protocol, with CFA and VFA. Two healthy volunteers were scanned to investigate the in vivo performance of each sequence (3T Siemens Verio, 32 channel head-coil). All scans used a spoiled-gradient echo 2D radial readout with 12 equally spaced spokes (TR 10 ms) per frame per ASL preparation, full Nyquist sampling (across multiple ASL preps), FOV 220 mm and single slice thickness 70 mm. Background-suppression involved pre-saturation followed by two FOCI pulses interleaved with the PCASL labeling to null static tissue at 100 ms before the first excitation.
Data at 1.15 mm2 in-plane resolution were acquired to compare CFA to VFA for both protocols. The sequential protocol used two averages to give matched noise averaging and scan-time: 2.5 min. Data at 0.63 mm2 in-plane resolution were acquired to better demonstrate differences in small distal vessel depiction (sequential used 2x over-sampling to give matched scan-times: 4.5 min).
Each acquired spoke was phase aligned to account for B0 drift before reconstructing offline using a non-uniform fast Fourier transform (NUFFT) with sampling density weighting,11 incorporating coil sensitivity information derived using the adaptive combine approach.12 Complex subtraction was performed before taking the magnitude.
Results and Discussion
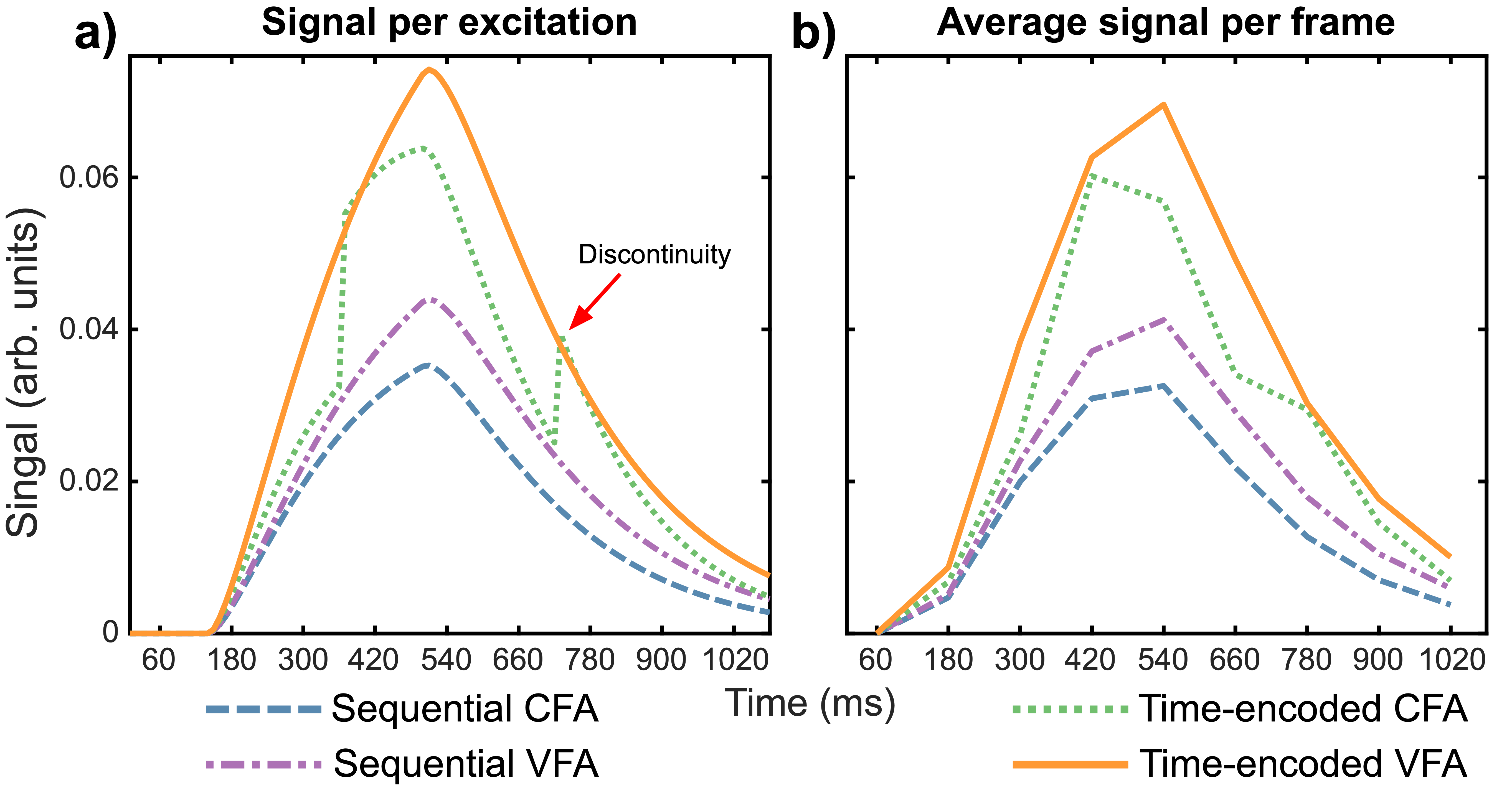
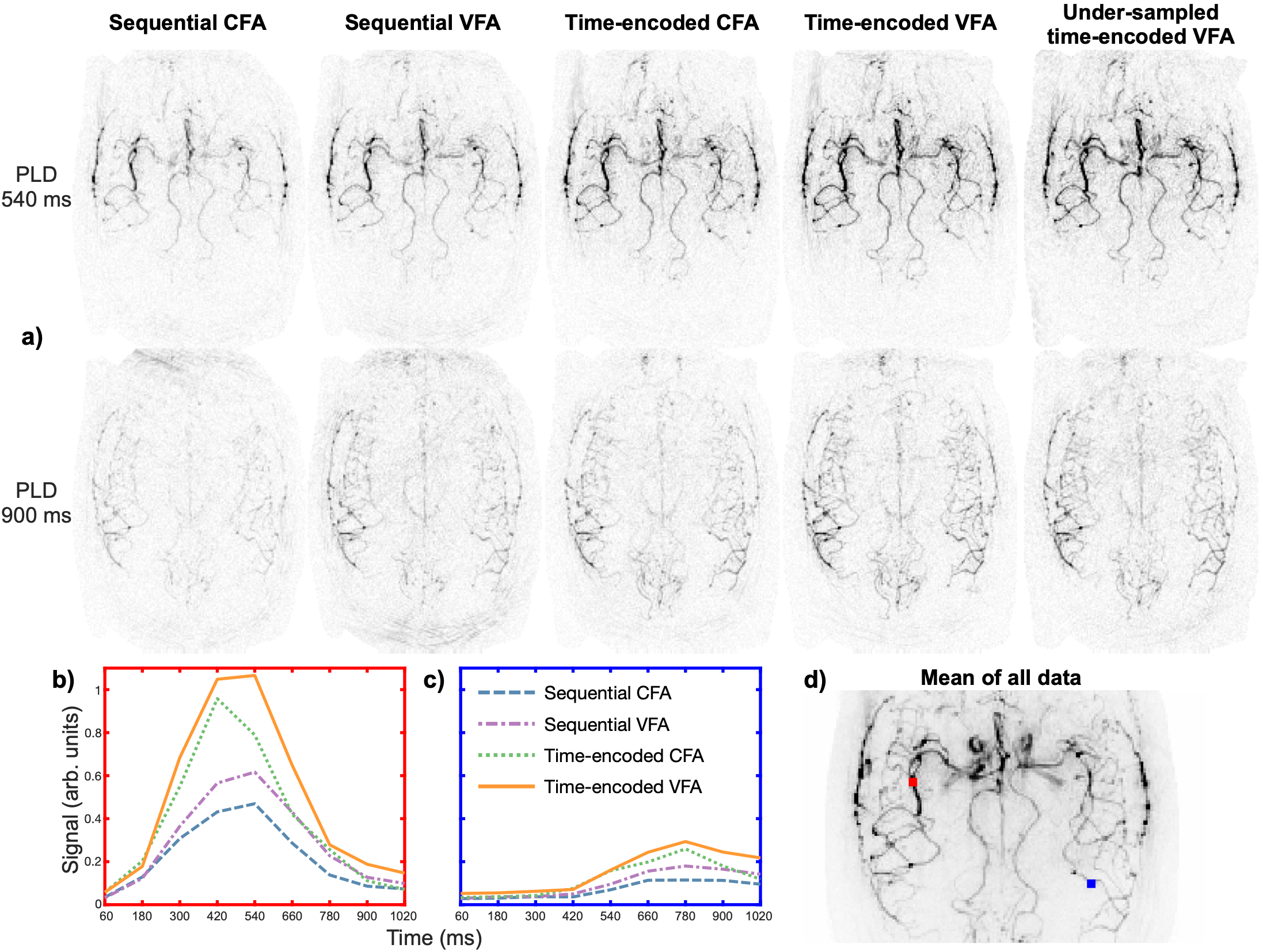
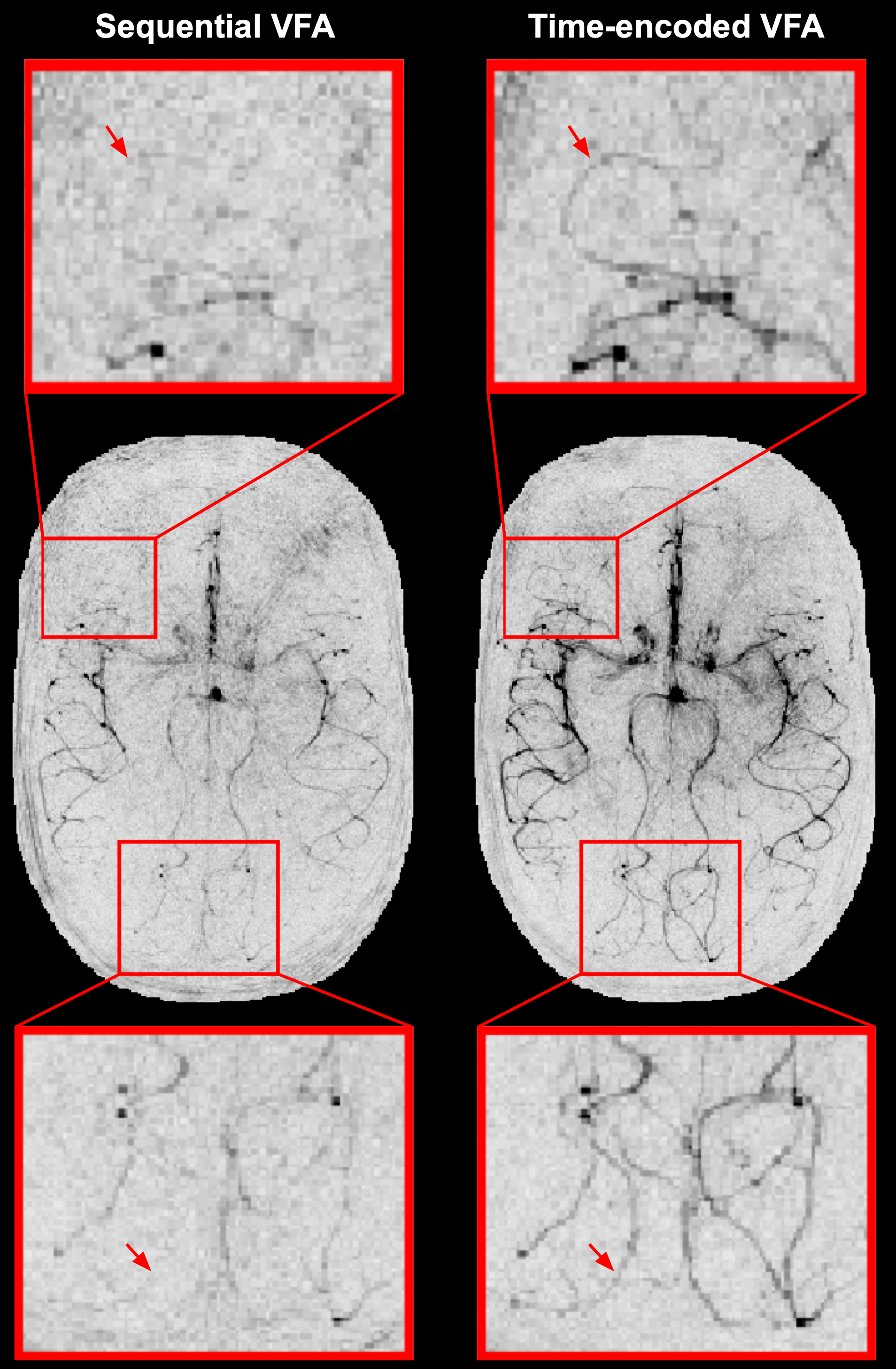
Figure 3 demonstrates the abrupt signal changes between images derived from different time-encoding blocks with CFA. Use of VFA removes these discontinuities, resulting in a smoother signal profile, and maximizes the ASL signal. Figure 4 demonstrates the in vivo signal improvement of the time-encoded VFA sequence over sequential and CFA variants. The higher resolution data in Figure 5 demonstrates that the time-encoded VFA sequence greatly improves the visual depiction of small distal vessels compared to the sequential VFA sequence.
One downside to using 3-block time-encoded PCASL is the need to acquire twice as many images as are necessary for sequential PCASL with a single average. This could be overcome by under-sampling the time-encoded data by a factor of 2, halving the scan-time. Under-sampling of such sparse angiograms with radial trajectories results in minimal noise-like artefacts.13,14 Acquired 2x under-sampled time-encoded data is also shown in Figure 4, demonstrating improved vessel depiction versus the sequential data, despite the halved scan-time and increase in noise.
Conclusion
These results suggest that using the proposed VFA scheme produces smoother time-courses with higher signal across the brain, which is particularly beneficial for depicting small distal vessels.
Future work includes validating the SNR improvement of under-sampled time-encoded VFA over fully-sampled sequential VFA and extension to a 3D acquisition.
Acknowledgements
This work was supported by funding from the Engineering and Physical Sciences Research Council (EPSRC), Medical Research Council (MRC) and the Royal Academy of Engineering [grant numbers: EP/L016052/1; EP/P012361/1; RF201617\16\23]. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z).References
1. Detre JA, Leigh JS, Williams DS, Koretsky AP. Perfusion imaging. Magn Reson Med 1992;23:37–45.
2. Williams DS, Detre JA, Leigh JS, Koretsky AP. Magnetic resonance imaging of perfusion using spin inversion of arterial water. Proc Natl Acad Sci 1992;89:212–216.
3. Dixon WT, Du LN, Faul DD, Gado M, Rossnick S. Projection angiograms of blood labeled by adiabatic fast passage. Magn Reson Med 1986;3:454–462.
4. Nishimura DG, Macovski A, Pauly JM, Conolly SM. MR angiography by selective inversion recovery. Magn Reson Med 1987;4:193–202.
5. Wang SJ, Nishimura DG, Macovski A. Multiple-readout selective inversion recovery angiography. Magn Reson Med 1991;17:244–251.
6. Schmitt P, Speier P, Bi X, Weale P, Mueller E. Non-contrast-enhanced 4D intracranial MR angiography: Optimizations using a variable flip angle approach. In: Proc. Intl. Soc. Mag. Reson. Med. 18. ; 2010. p. 402.
7. Günther M. Highly efficient accelerated acquisition of perfusion inflow series by Cycled Arterial Spin Labeling. In: Proc. Intl. Soc. Mag. Reson. Med. 15. ; 2007. p. 380.
8. van der Plas MCE, Schmid S, Versluis M, van Osch MJP. Time-encoded golden angle radial ASL. In: Proc. Intl. Soc. Mag. Reson. Med. 26. ; 2018. p. 0306.
9. Suzuki Y, Teeuwisse WM, Schmid S, Helle M, Cauteren M Van, Osch MJP Van. Improving 4D pCASL angiography by combining Hadamard time-encoding with Look-Locker readout. In: Proc. Intl. Soc. Mag. Reson. Med. 22. ; 2014. p. 6460.
10. Okell TW, Chappell M a., Schulz UG, Jezzard P. A kinetic model for vessel-encoded dynamic angiography with arterial spin labeling. Magn Reson Med 2012;68:969–979.
11. Fessler JA, Sutton BP. Nonuniform fast fourier transforms using min-max interpolation. IEEE Trans Signal Process 2003;51:560–574.
12. Walsh DO, Gmitro AF, Marcellin MW. Adaptive reconstruction of phased array MR imagery. Magn Reson Med 2000;43:682–690.
13. Wu H, Block WF, Turski PA, Mistretta CA, Johnson KM. Noncontrast-enhanced three-dimensional (3D) intracranial MR angiography using pseudocontinuous arterial spin labeling and accelerated 3D radial acquisition. Magn Reson Med 2013;69:708–715.
14. Okell TW. Combined angiography and perfusion using radial imaging and arterial spin labeling. Magn Reson Med 2018. doi: 10.1002/mrm.27366.
Figures