0387
A MR-based nomogram for predicting cerebral palsy in periventricular leukomalacia children before 2 years old1The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China, 2The First Affiliated Hospital of Henan University of traditional Chinese Medicine, Zhengzhou, China, 3Xi’an Children Hospital, Xi'an, China, 4GE Healthcare, Bei Jing, China
Synopsis
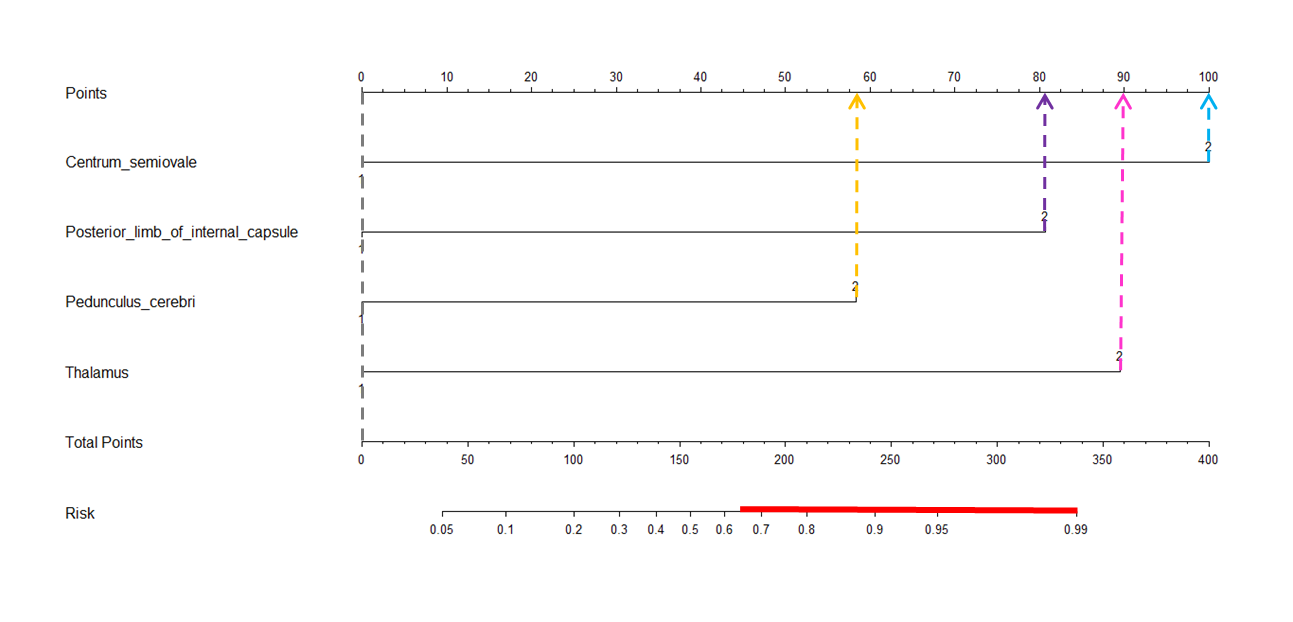
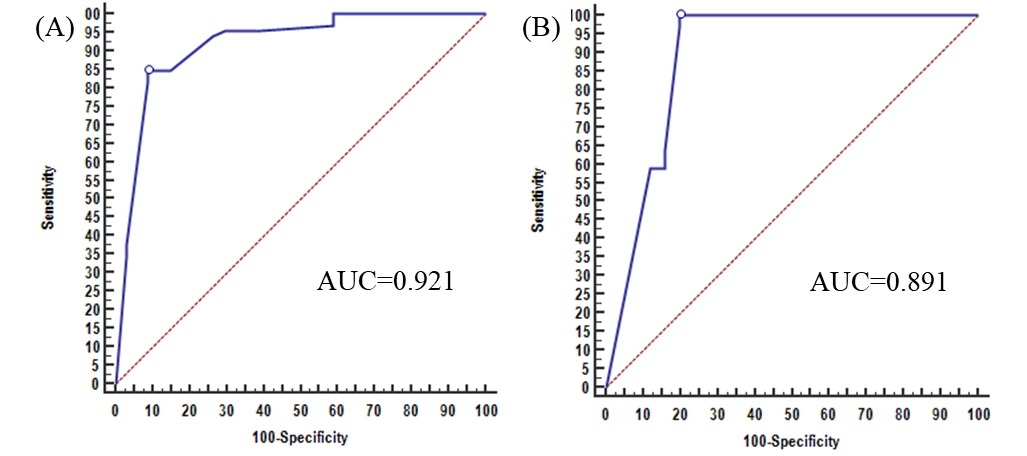
Early identification of cerebral palsy (CP) in children with periventricular leukomalacia (PVL) is crucial for prescribing the indispensable treatment and rehabilitation. In this study, we visually assessed PVL-associated MR signs, i.e. T2/T2 Flair hyperintense in the centrum ovale, posterior limb of internal capsule, pedunculus cerebri and thalamus, and found they were independent predictors of CP. Based on these signs, a MR-based nomogram for predicting CP in PVL children aged less than 2 yr was developed. Results indicated that the area under receiver operating characteristic curve, sensitivity and specificity for this nomogram were 0.921, 91.2% and 83.3%, respectively. These suggested the potential role of our MR nomogram in predicting the CP outcome of PVL children before 2 years old.
Introduction
Periventricular leukomalacia (PVL) is a serious sequelae of brain white matter injury, and is a major cause of cerebral palsy (CP) 1. Early identification of CP in PVL children is crucial for prescribing the indispensable treatment and rehabilitation. However, current diagnosis of CP is always determined at 2 yr of age or older2. This posed more difficulty for efficient treatment and rehabilitation. Previous studies3,4 reported the various PVL-associated MR features; among them, some were suggested as potential biomarkers in CP prediction. However, a clinically-practical prediction method remains absent. To address such issue, we visually assessed series of PVL-associated MR signs and explored their ability in predicting risk of CP. Then, a MR-based nomogram for predicting CP was developed to serve for early identification of CP risk in PVL children aged less than 2 yr.Methods
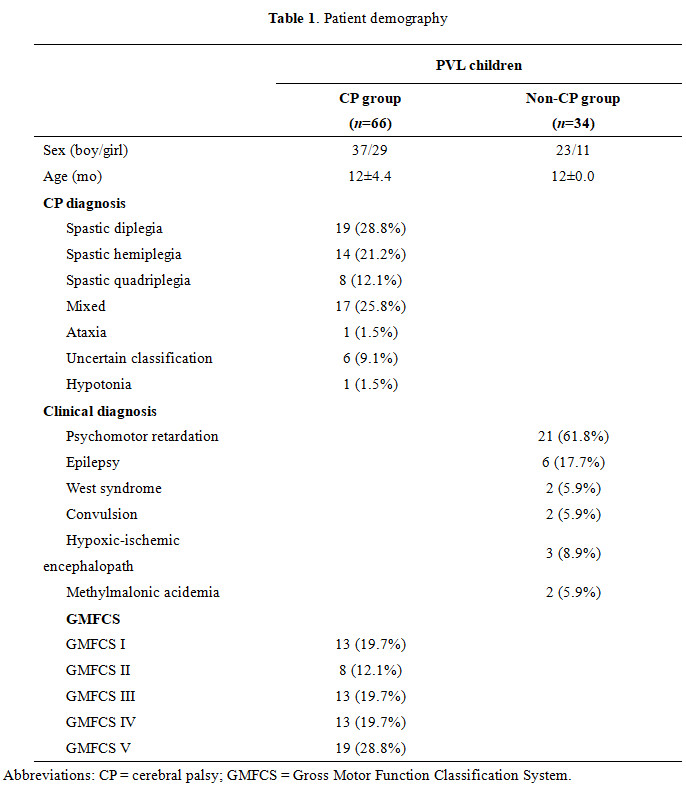
Between April 2013 and April 2018, 100 PVL3,5 children aged less than 2 yr (boy/girl, 60/40; age, 4~23 mo) underwent conventional MRI were retrospectively enrolled from department of radiology of the first author’s affiliation. All the children were followed up until 2 yr and CP diagnosis were clear6. According to CP diagnosis, all children were divided into PVL CP (n=66) and PVL non-CP (n=34) groups. MR signs (T2/T2 Flair hyperintense in the centrum ovale, posterior limb of internal capsule [PLIC], pedunculus cerebri and thalamus) were assessed by a visually scoring method, and were evaluated for predicting CP based on a binary logistic regression (Figure 1). 10-folded cross validation was employed to evaluate the prediction model. In addition to 100 subjects, 64 children were included for independent verification. The overall ability of predictive nomogram to discriminate between CP and non-CP was analyzed using a binary receiver operating characteristic (ROC) regression analysis and quantified using the areas under the ROC curves (AUC). P<0.05 indicated that the difference was statistically significant. Analyses were performed with software SPSS 20.0 for IBM (SPSS Inc. Chicago, IL, USA), MedcCalc (ver 13.0.0.0, bvba) and R software (ver 3.4.0, USA).Results
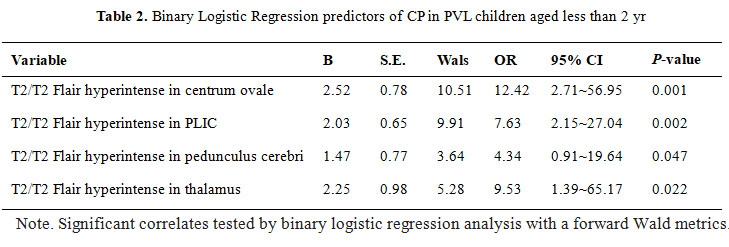
Demographic, clinical variables for the study cohort (100 children) are depicted in Table 1. No significant difference was found between CP and non-CP groups in terms of sex and age. Results indicated that AUC, sensitivity and specificity of MR nomogram were 0.921 (95% CI: 0.845~0.963), 91.2% and 83.3%, respectively. Those of 10-fold cross-validation were 0.814 (95% CI: 0.715~0.933), 90.1% and 81.5%, while those in the verification were 0.891 (95% CI: 0.788-0.955), 100% and 80.0%. (Figure 2) For MR signs, the binary logistic regression indicated that T2/T2 Flair hyperintense in the centrum ovale (odds ratio [OR]=12.416, P=0.001), PLIC (OR=7.631, P=0.002), pedunculus cerebri (OR=4.341, P=0.047) and thalamus (OR=0.950, P=0.022) were the independent risk predictors of CP (Table 2).Discussion
In this study, we developed a practical MR nomogram to predict the probability of CP in PVL children before 2 years old by assessing several MR signs. We demonstrated that the newly MR nomogram performed better than previous models7,8, suggesting prospective value of image-based analysis in CP outcome prediction of PVL children. The role of MRI in predicting CP has been previously studied9,10. By comparison, we found that T2/T2 Flair hyperintense in centrum semiovale, PLIC, pedunculus cerebri and thalamus presented higher ability in risk prediction of CP. Among these, centrum semiovale, PLIC, pedunculus cerebri located in the centralized walking area of corticospinal tract. In particular, lesions in PLIC and pedunculus cerebri have been demonstrated to show close link with dyskinesia in CP children. In this regard, abnormal MR findings of PVL in these regions may be considered as risk predictors. Besides, severe PVL also involved the occipital part of the thalamus11. Thalamus plays critical roles in motor and postural control and locomotion. Therefore, the thalamic damage affects motor control and indirectly leads to motor dysfunction, e.g. CP.Conclusion
The MR-based nomogram for CP prediction showed potential role in early prediction of CP risk in PVL children aged less than 2 yr.Acknowledgements
This work was supported by the National Key Research and Development Program of China (2016YFC0100300), National Natural Science Foundation of China (No.81171317, 81471631), and the 2011 New Century Excellent Talent Support Plan of the Ministry of Education, China (NCET-11-0438).References
1. Rutherford MA.Supramaniam V,Ederies A, et a1.Magnetic resonance imaging of white matter diseases of prematurity. Neuroradiology. 2010; 52 (6): 505-521.
2. Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy. Dev Med Child Neurol. 2007; 109:8-14.
3. Imamura T, Ariga H, Kaneko M, et al. Neurodevelopmental outcomes of children with periventricular leukomalacia. Pediatrics and Neonatology. 2013; 54(6):367-72.
4. Slaughter LA, Bonfante-Mejia E, Hintz SR,et al. Early Conventional MRI for Prediction of Neurodevelopmental Impairment in Extremely-Low-Birth-Weight Infants. Neonatology 2016;110(1):47-54. 5. Zubiaurre-Elorza L, Soria-Pastor S, Junque C, et al. Gray matter volume decrements in preterm children with periventricular leukomalacia. Pediatric research. 2011; 69(6): 554-60.
6. Palisano R, Rosenbaum P, Walter S, Russell D, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;39(4):214-23.
7. George JM, Boyd RN, Colditz PB, et al.PPREMO: a prospective cohort study of preterm infant brain structure and function to predict neurodevelopmental outcome. BMC Pediatr. 2015 ;16;15:123.
8. Van der Aa NE, Verhage CH, Groenendaal F, et al. Neonatal neuroimaging predicts recruitment of contralesional corticospinal tracts following perinatal brain injury. Dev Med Child Neurol 2013;55(8):707-12.
9. Woodward LJ, Anderson PJ, Austin NC, Howard K, et al. Neonatal MRI to predict neurodevelopmental outcomes in preterm infants. N Engl J Med 2006;355(7):685-94.
10. Slaughter LA, Bonfante-Mejia E, Hintz SR,et al. Early Conventional MRI for Prediction of Neurodevelopmental Impairment in Extremely-Low-Birth-Weight Infants. Neonatology 2016;110(1):47-54.
11. Yokochi K. Thalamic lesions revealed by MR associated with periventricular leukomalacia and clinical profiles of subjects. Acta Paediatr. 1997; 86(5): 493-496.
Figures