0080
Exploring static and dynamic functional connectivity differences between cognitively impaired and non-impaired active professional fighters1Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, United States, 2University of Colorado Boulder, Boulder, CO, United States
Synopsis
Both static and dynamic FC differences between cognitively impaired and non-impaired active fighters were explored using resting-state fMRI. Reduced network strength in anterior default mode network and cerebellar network were observed in impaired fighters, as compared to the non-impaired fighters. Four dynamic FC states were identified with k-means clustering and abnormities in state 2 were observed in impaired fighters. Higher classification accuracy was obtained using dynamic FC matrices as input features to a non-linear classifier, as compared to using static FC matrices as input features, which demonstrates that the time-varying brain activities carry richer cognitive impairment-related information.
Introduction.
Previous studies have shown that active professional fighters who experience repeated head trauma may suffer from cognitive impairment when compared to age matched healthy controls1,2. Previous neuroimaging studies have identified abnormalities in brain regional volumes, cortical thickness and structural connectivity in cognitively impaired active fighters, which correlate with their cognitive task performances3,4. However, functional connectivity (FC) changes in active fighters remain unclear and dynamic functional connectivity abnormalities in active fighters have not yet been investigated. Here we explored both static and dynamic functional connectivity differences between cognitively impaired and non-impaired active fighters using resting-state fMRI.Methods.
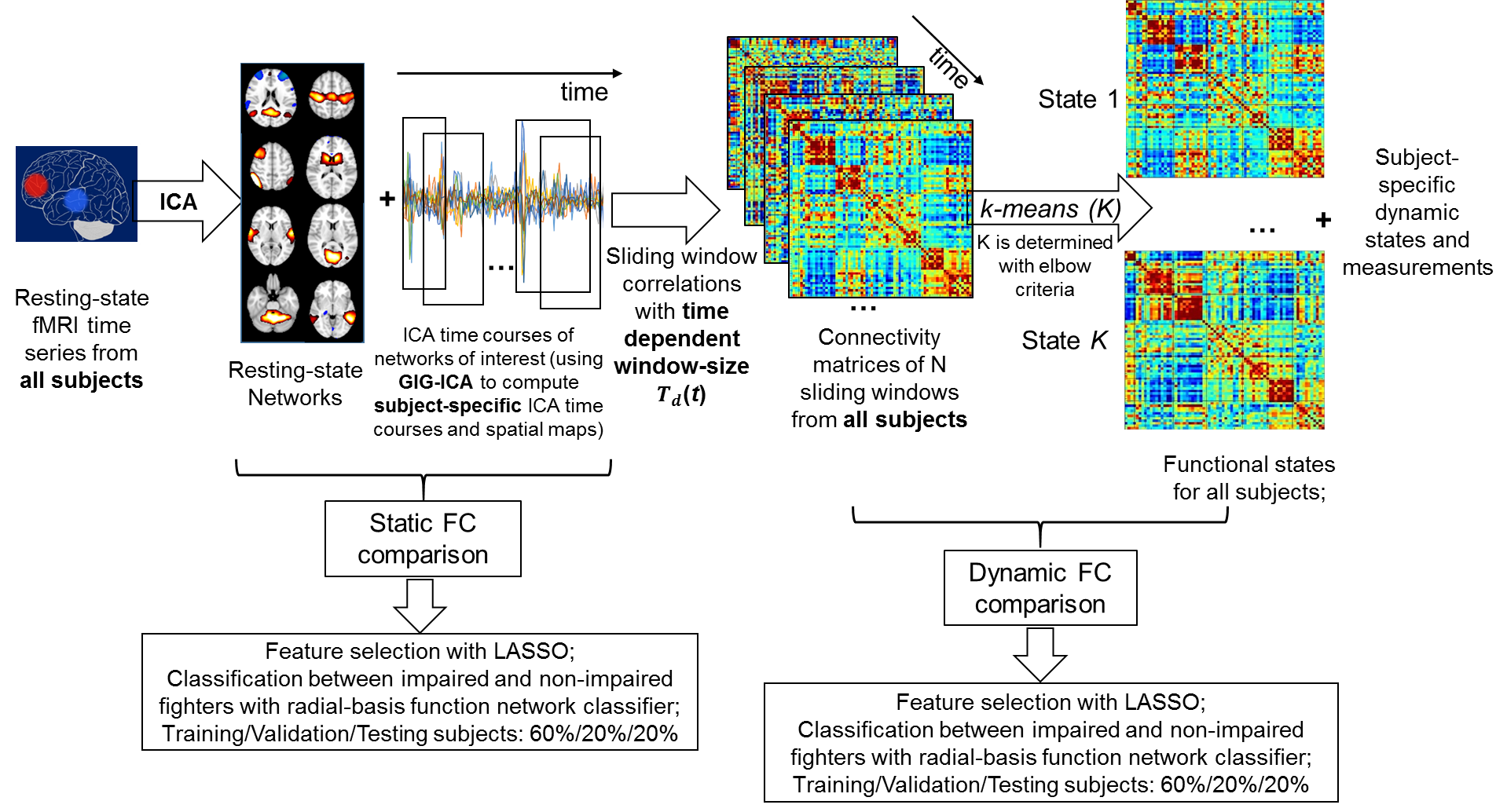
Subjects. A total of 252 active professional fighters were recruited at our center as part of the Professional Fighters Brain Health Study2. Each subject went through neuropsychological assessments to measure psychomotor speed (PSY) and processing speed (P). 68 subjects were classified as cognitively impaired based on their PSY and P scores being 1.5 standard deviation below the average5 (65Males, age=29.80±6.20 years, years of education (YOE)=13.03±2.12 years). 65 matched non-impaired fighters (58Males, age=28.78±5.27 years, YOE=13.28±1.63 years) were selected and also included in the analysis. Resting-state fMRI data were collected for all subjects on a 3T Siemens scanner (TR/TE/resolution=2.8s/28ms/2x2x4mm3, 30 slices, axial acquisition, 137 time frames). Static functional connectivity analysis. After standard preprocessing steps, fMRI data from all subjects were normalized to the standard MNI-152 2mm template. Functional brain networks were obtained through group independent component analysis (ICA). Out of 100 ICA components, 48 components were identified as resting-state networks. Subject-specific spatial maps and time-courses for each network were reconstructed using GIG-ICA6. Spatial maps of each network were compared between impaired and non-impaired fighters. Functional connectivity among different networks (FC matrices) were computed using the correlation of the subject-specific time-courses between each network pairs. FC matrices were finally compared between impaired and non-impaired fighters. Dynamic functional connectivity analysis. Dynamic FC was estimated using a sliding-window method7, with the optimum window-size computed through empirical mode decomposition method8. Dynamic FC matrices, i.e. correlation matrices among different networks, were computed within each window and a k-means clustering was further carried out to compute dynamic FC states. Number of dynamic states was determined with the elbow criteria. Subject-specific dynamic FC matrices for each state were further computed by averaging the FC matrices of all windows clustered to the state. The dynamic FC matrices were also compared between impaired and non-impaired fighters for each state. Classification. Automated feature selections (using LASSO9) and classifications (using radial basis function classifier)10 were finally carried out using static FC matrices and dynamic FC matrices of all states as input features, separately.Results.
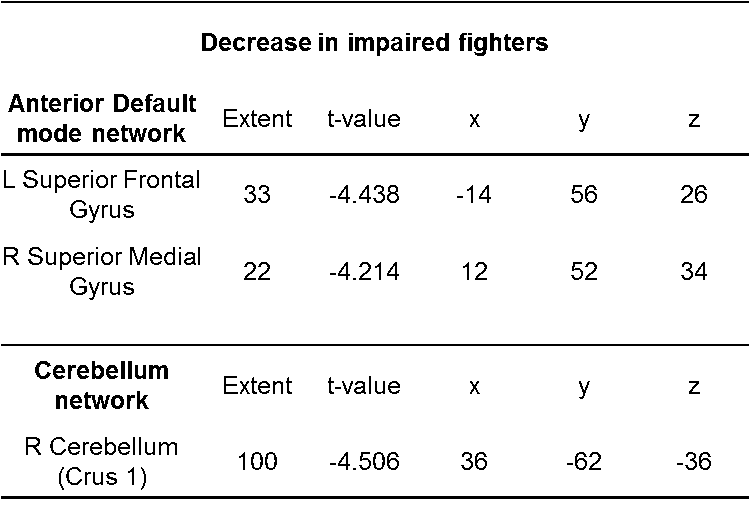
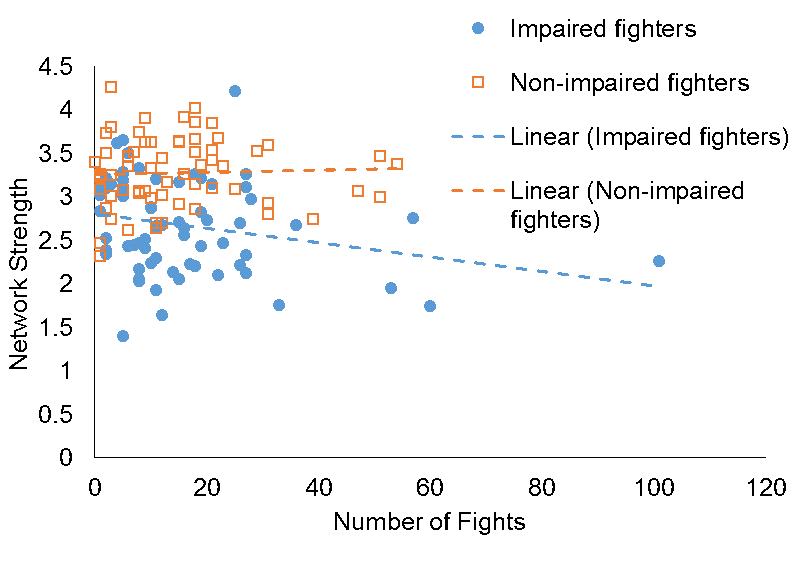
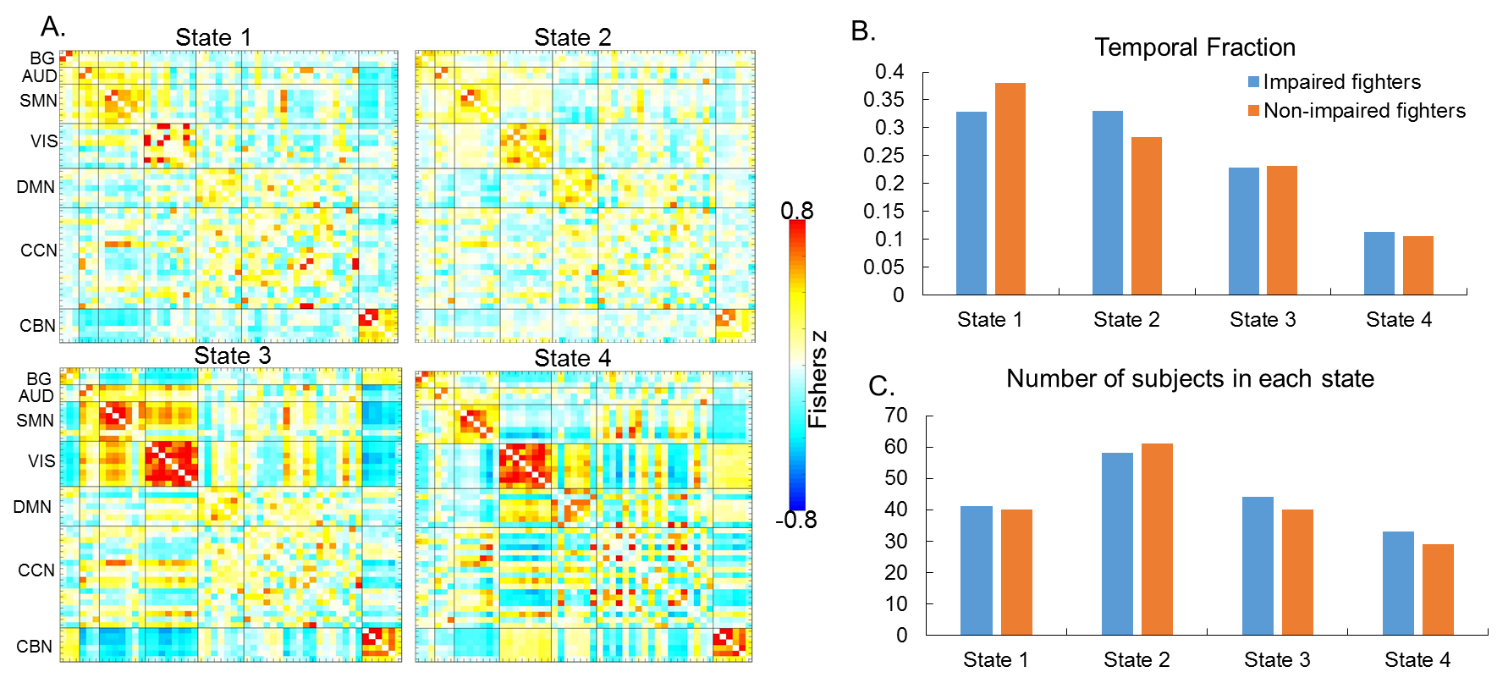
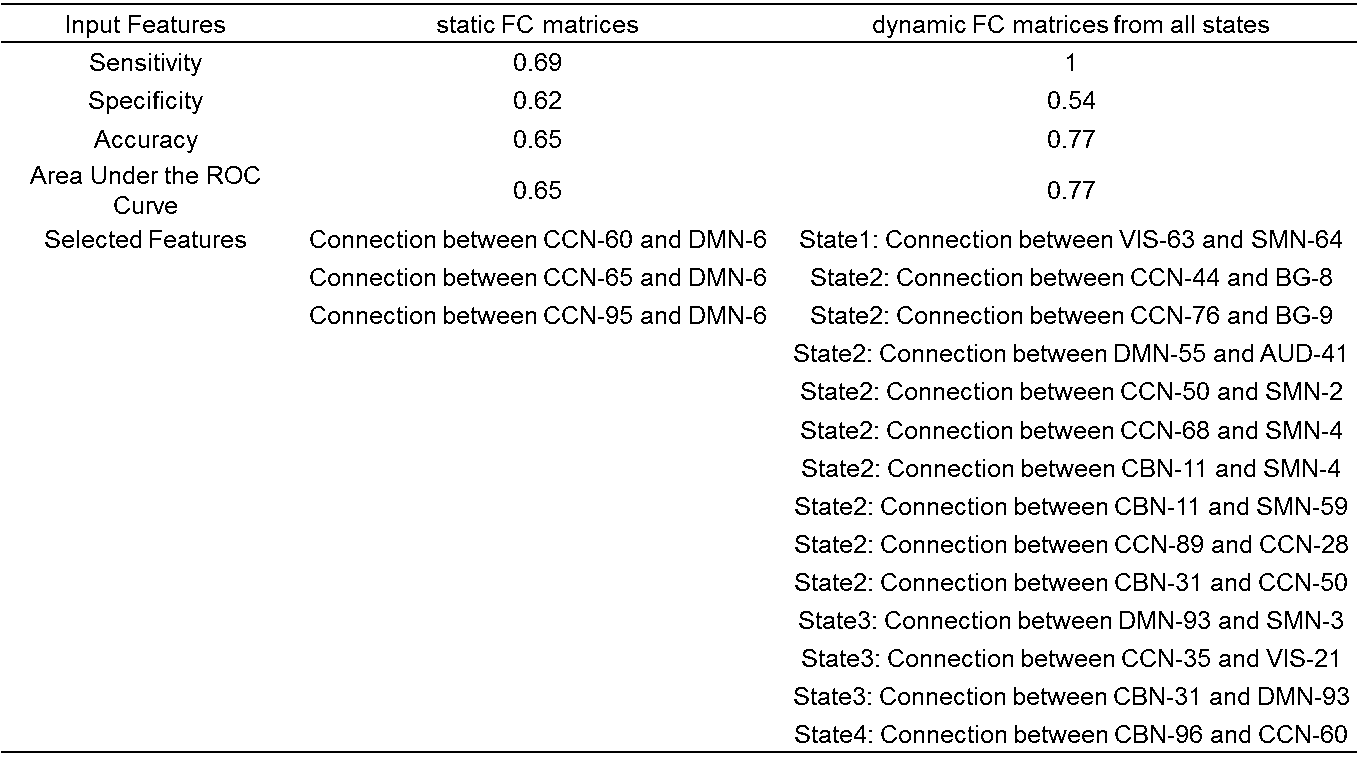
Fig.1 describes the flowchart used in the analysis. Static network comparison. In the anterior default mode network (DMN) and cerebellum network, significant decreased network strengths are observed in impaired fighters (p<0.05, FDR corrected), with the cluster center located at the superior frontal gyrus and cerebellum crust1, respectively (Table. 1). The reduced network strength in anterior DMN is negatively correlated with the number of fights in all fighters (p=0.03, Fig. 1), adjusted for the age, gender and YOE. Static FC comparison. No significant between network difference is observed in the static FC comparison at FDR corrected p<0.05. Dynamic FC comparison. Four dynamic functional states were identified (Fig. 2(A)) and impaired fighters spent more time (but not significant, Fig 2(B)) in a weakly connected state 2. In this state (state 2), impaired fighters showed reduced functional connections between cognitive control networks and motor networks (p<0.001), and increased functional connections between cerebellum networks and motor networks (p<0.001), as compared to non-impaired fighters. Classification. Table 2 lists the selected features using LASSO and the accuracy of classifying impaired and non-impaired fighters in the independent testing set. The accuracy was 0.65 when using static FC matrices as features and 0.77 when using dynamic FC matrices as features.Discussions and conclusions.
The higher classification accuracy with dynamic FC as features suggests the time-varying brain activities carry richer cognitive impairment-related information. This study is the first attempt to investigate abnormalities in both static and dynamic FC of cognitively impaired active fighters, which provides evidence of both disrupted static functional networks and altered dynamic functional connections in impaired active professional fighters.Acknowledgements
The study is supported by the National Institutes of Health (grant number 1R01EB014284 and P20GM109025), grants from Lincy Foundation, the Peter and Angela Dal Pezzo funds and the young scientist award at CCLRCBH.References
[1]. Banks et al., 2014. Impulsiveness in Professional Fighters. J. Neuropsychiatry Clin. Neurosci.
[2]. Bernick et al., 2013. Professional fighters brain health study: Rationale and methods. Am. J. Epidemiol.
[3]. Koerte et al., 2015. A review of neuroimaging findings in repetitive brain trauma. Brain Pathol.
[4]. Mishra et al., 2017. Multimodal MR Imaging Signatures of Cognitive Impairment in Active Professional Fighters. Radiology.
[5]. Schinka et al., 2010. Defining mild cognitive impairment: impact of varying decision criteria on neuropsychological diagnostic frequencies and correlates. Am. J. Geriatr. Psychiaty.
[6]. Du and Fan, 2013. Group information guided ICA for fMRI data analysis. Neuroimage.
[7]. Allen, et al., 2014. Tracking whole-brain connectivity dynamics in the resting state. Cereb. Cortex
[8]. Cordes, D et al., 2018. Advances in functional magnetic resonance imaging data analysis methods using Empirical Mode Decomposition to investigate temporal changes in early Parkinson’s disease. Alzheimer’s Dement. Transl. Res. Clin. Interv.
[9]. Tibshirani R., 1996. Regression Shrinkage and Selection via the Lasso. Journal of the Royal Statistical Society.
[10].Zhuang et al., 2016. A combinatorial model approach for feature selection from multimodal MRI data. ISMRM.
Figures