Liver Fat, Iron, & Fibrosis Abbreviated Protocols
1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
With the emergence of non-alcoholic fatty liver disease (NAFLD) as most common chronic liver disease, detection and quantification of liver fat and fibrosis becomes important. Iron overload frequently seen in association with fatty liver and liver fibrosis. Noninvasive quantification of liver fat, iron and fibrosis with MRI is now considered the standard for diagnosis and monitoring. In this presentation, typical clinical scenarios that requires MRI abbreviated protocol for liver fat, iron and fibrosis quantification, candidate sequences and multi-parametric MRI protocols will be discussed. MRI protocols will be illustrated with clinical examples and limitations will be highlighted.
Outcome/Objectives
At the end of this lecture,the participant will be able to
- Understand the clinical scenarios that require abbreviated protocol for hepatic fat, iron and fibrosis
- Learn about multi-parametric MRI protocols
- Understand the limitations of abbreviated protocol
Background
Non-alcoholic fatty liver disease is the leading cause of chronic liver disease (CLD), hepatocellular carcinoma and liver transplantation in the world. NAFLD has a spectrum of relatively benign non-progressive non-alcoholic fatty liver (NAFL) to progressive nonalcoholic steatohepatitis (NASH) which would finally lead to fibrosis or cirrhosis. Physicians evaluating the patients at risk of NAFLD (obesity, diabetes, and metabolic syndrome) would first confirm the diagnosis of NAFLD, then determine NASH vs. NAFL and finally assess the severity of hepatic fibrosis. Fibrosis is the most important prognostic factor in NAFLD patients and advanced fibrosis (≥ stage 3) carry worse prognosis. Increased iron deposition commonly occurs in many CLD including NAFLD. Quantifying Liver iron content (LIC) is important for confirmation of hereditary hemochromatosis (HH) in patients with genetic predisposition and for management decisions in known HH patients. LIC is also important in patients with iron overload due to transfusions or hematologic disorders for decisions on chelation therapy. Liver fibrosis is the end-stage healing response to injury in CLDs and the outcome depends on fibrosis stage. Early detection is of paramount importance as anti-fibrotic treatment would be most effective at earlier stages of liver fibrosis. Monitoring progression and response to anti-fibrotic treatment are invaluable in the follow up of CLD patients.Typical clinical scenarios for abbreviated liver quantification protocol
- Living liver transplant donor
- Detection and quantification of fat, iron and fibrosis in patients with risk factors
- Assessment of response to treatment or interventions
- Clinical trials
- Patient factors- mild claustrophobia, chronic disability, spine issues, etc
Ideal abbreviated Protocol
- Reduced scan time (time is money!)- A breath hold sequence would be great
- Simple to perform- set up, running the sequence, minimum post processing
- Proven clinical utility and diagnostic accuracy
- Low failure rate/recalls
- No need for intravenous contrast
Candidate sequences for abbreviated protocol
Fat
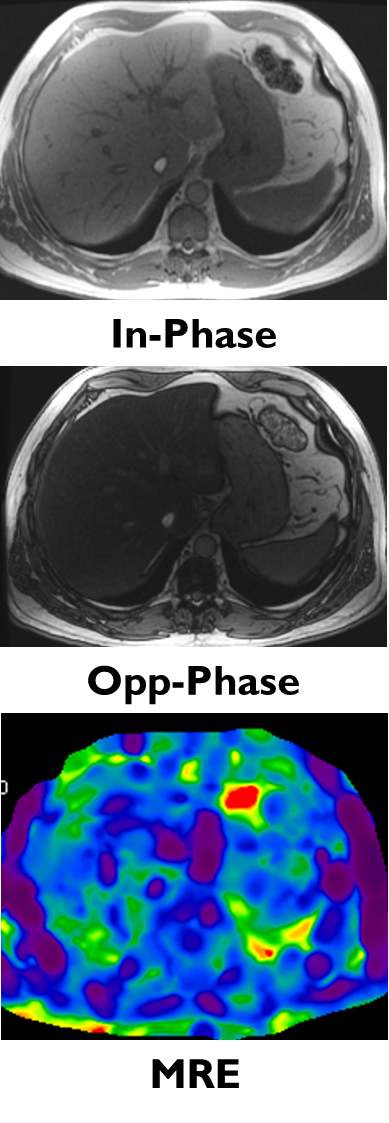
- Conventional In/Opp sequence; 2D or 3D dual echo
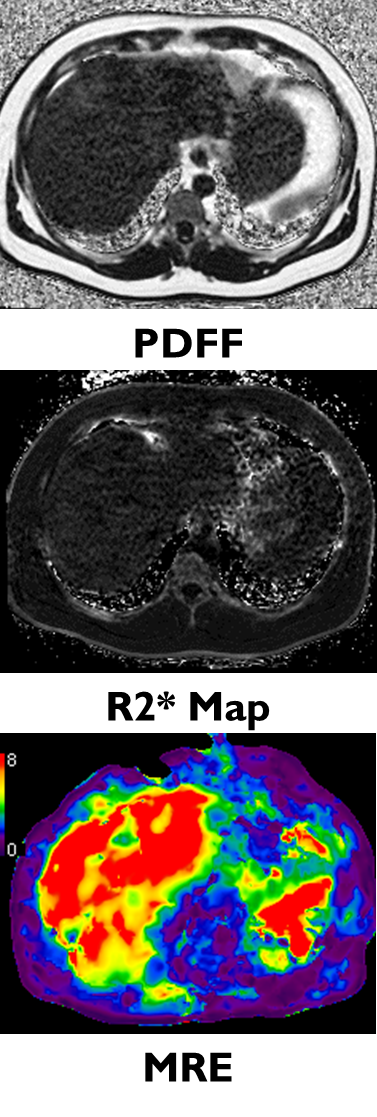
- Chemical shift based Proton density fat fraction calculation (PDFF)
Iron
- Signal intensity ratio
- R2* Relaxometry
Fibrosis
- MR Elastography
- Liver T1-mapping
- Diffusion weighted imaging and ADC
Multi-parametric protocol examples
- Localizer + 2D/3D dual echo + MRE: liver fat detection and rule out steatohepatitis +/- fibrosis
- Localizer + IDEAL + MRE: liver fat, iron and fibrosis quantification
- Localizer + T1 map+ T2*+ PDFF: liver fat, iron and LIF marker quantification
Limitations
- Potentially miss focal liver lesions such as HCC developing in background of liver fibrosis
- Limited evaluation of portal hypertension features particularly esophageal varices that have potential to bleed with high mortality
Acknowledgements
No acknowledgement found.References
- Villar-Gomez E and Chasalani N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J Hepatology 2018; 68:305-315.
- Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol hepatol 2013;10: 686-90.
- Reeder SB, Cruite I, Hamilton G, Sirlin CB. Quantitative assessment of liver fat with magnetic resonance imaging and spectroscopy. J Magn Reson Imaging 2011; 34:729-749.
- Liu CY, Mckenzie CA, Yu H, Brittain JH, Reeder SB. Fat quantification with IDEAL gradient echo imaging: correction of bias from T(1) and noise. Magn Reson Med 2007;58:354-364
- Yu H, Shimakawa A, McKenzie CA, Brodsky E, Brittain JH, Reeder SB. Multiecho water-fat separation and simultaneous R2* estimation with multifrequency fat spectrum modeling. Magn Reson Med 2008; 60:1122-1134.
- Reeder SB, Hu HH, Sirlin CB. Proton density fat-fraction: a standardized MR-based biomarker oftissue fat concentration. J Magn Reson Imaging 2012; 36:1011-1014.
- Tang A, Tan J, Sun M, Hamilton G, Bydder M, Wolfson T, Gamst AC, et al. Nonalcoholic fatty liverdisease: MR imaging of liver proton density fat fraction to assess hepatic steatosis. Radiology2013; 267:422-431Labranche R, Gilbert G, Cerny M, Vu KN, Olivie D, Billiard JS, Yokoo T, Tang A. Liver Iron quantification with MR imaging: A Primer for Radiologists. Radiographics 2018; 38:392-412.
- Venkatesh SK, Yin M, Ehman RL. Magnetic resonance elastography of liver: technique, analysis, and clinical applications. J Magn Reson Imaging. 2013 Mar;37(3):544-55. doi: 10.1002/jmri.23731.
- Venkatesh SK, Yin M, Ehman RL.Magnetic resonance elastography of liver: clinical applications.J Comput Assist Tomogr. 2013 Nov-Dec;37(6):887-96.
- Wang J, Glaser KJ, Zhang T, Shan Q, He B, Chen J, Yin M, Dzyubak B, Kugel JL, Kruse SA, Grimm RC, Venkatesh SK, Ehman RL. Assessment of advanced hepatic MR elastography methods for susceptibility artifact suppression in clinical patients. J Magn Reson Imaging. 2018 Apr;47(4):976-987
- Banerjee R, Pavlides M, Tunnicliffe EM, Piechnik SK, Sarania N, Philips R, Collier JD, Booth JC, Schneider JE, Wang LM, Delaney DW, Fleming KA, Robson MD, Barnes E, Neubauer S. Multiparametric magnetic resonance for the non-invasive diagnosis of liver disease. J Hepatol. 2014 Jan;60(1):69-77.
Figures