Current State of the Art
1NYU Langone Medical Center, United States
Synopsis
Abdominal or Body MRI suffers from number of limitations such as (1) slow and inefficient acquisition (2) sensitivity to motion related artifacts and (3) limited volumetric coverage and spatial resolution which are constrained by the breath-hold capacity of the patients.
Various methods are used clinically and are being investigated to overcome these limitations in order to permit motion robust and rapid imaging of the abdomen. This talk will briefly discuss some of these methods for (1) fast imaging and (2) motion compensated imaging of the abdomen.
ISMRM 2018 Weekend Course - Body MRI: Realities & Controversies Session # WE-03A
Title: Current State of the Art
Abdominal or Body MRI suffers from number of limitations such as (1) slow and inefficient acquisition (2) sensitivity to motion related artifacts and (3) limited volumetric coverage and spatial resolution which are constrained by the breath-hold capacity of the patients. It is important to understand how MRI images are acquired, what contributes to the acquisition time and how we can manipulate acquisition schemes to address above stated limitations.
Target Audience: Radiologists, MRI technologists, residents
Objectives: 1. Understand basic concepts of k-space and acquisition time. 2. Discuss various methods to accelerate acquisition by k-space undersampling. 3. Discuss motion robust schemes including non-Cartesian k-space sampling.
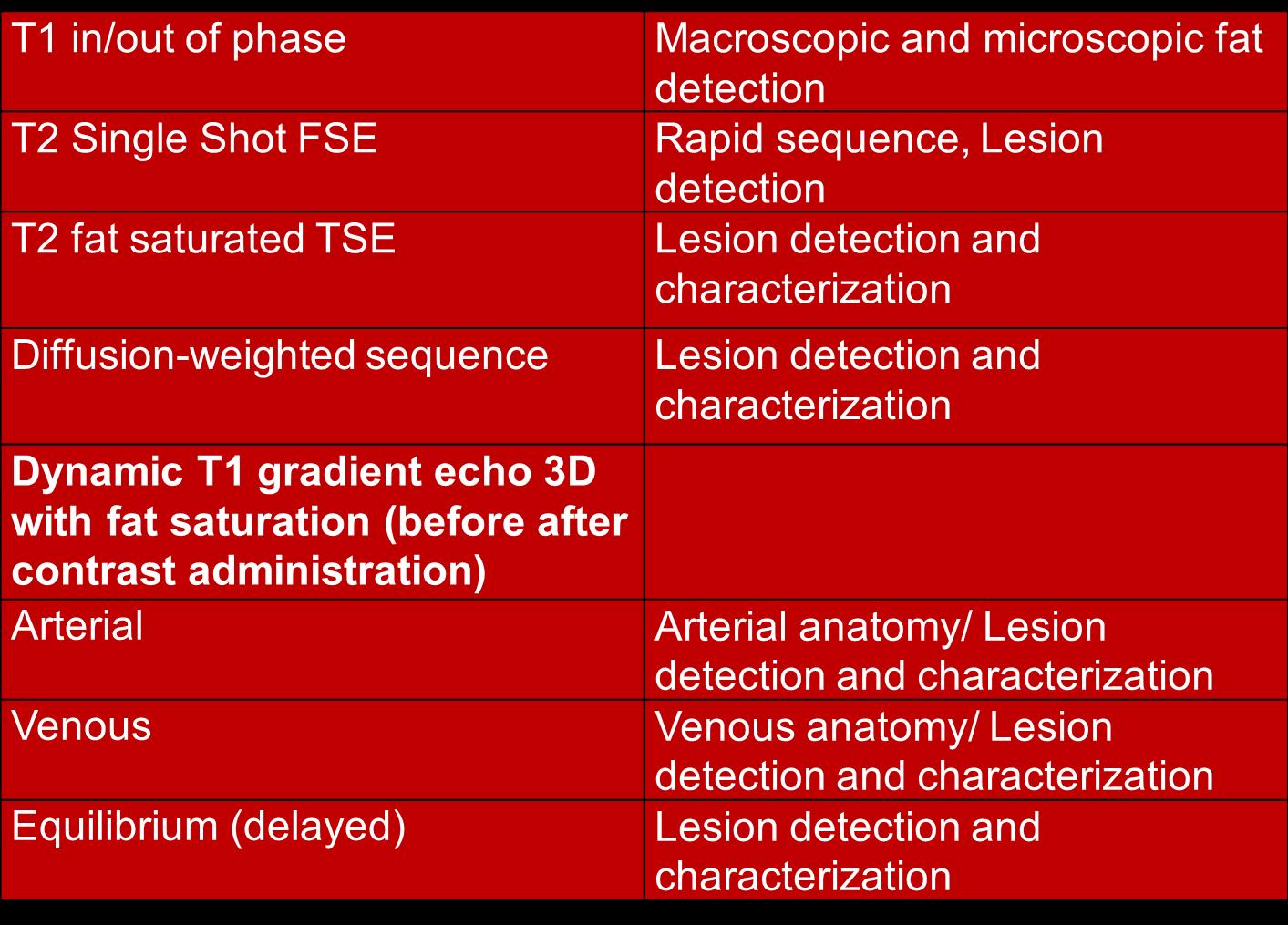
Introduction: Routine/Generic protocol for MRI examination of the abdomen (liver) is shown below (Figure 1). Routine MRI protocol of the abdomen/liver is usually designed to provide high spatial resolution as well as high temporal resolution for lesion detection and characterization.
Problem with current acquisition schemes: Many of these acquisitions are performed in breath-hold and in a sequential fashion. This is inefficient and results in suboptimal image quality when patients (such as sick, elderly, and pediatric) are unable to suspend their respiration during image acquisition.
Potential Solutions: To overcome these challenges, we will examine 2 approaches that can be implemented clinically.
Approach # 1: Increase speed to decrease breath-hold (fast imaging)
Approach # 2: Compensate for motion (in prospective or retrospective manner)
Approach # 1: Fast Imaging: Increase speed to decrease breath-hold.
There are number of methods that are available on almost all current MRI systems to “speed-up” the MR examination. We will briefly discuss following methods which are either being routinely used or are being actively investigated for abdominal imaging, especially for contrast enhanced T1-weighted dynamic imaging.
- Parallel Imaging
- View Sharing or time resolved techniques
- Compressed Sensing
All of these methods permit undersampling of the k-space data and reconstruction of images from the under-sampled data. As less of the k-space data is being acquired, this results in faster imaging and shorter duration of the breath-holds.
Approach #2: Motion compensated imaging
Another option is to permit patients to breath freely (without breath-holding) and account for respiratory motion either in a prospective or retrospective manner to generate motion robust imaging. These techniques are more commonly employed for T2W imaging as well as Diffusion Weighted Imaging (DWI) in the abdomen. Following methods will be discussed:
- Multiple acquisitions or averages (no navigator)
- Navigators (External and MR based)
- Self-navigation with focus on non-Cartesian acquisition schemes
These methods usually require oversampling of k-space or acquisition of the data during a particular phase of the respiratory cycle. Therefore, these methods tend to increase acquisition time. Novel methods that extract respiratory motion directly, including from non-Cartesian k-space acquisition and reconstruct motion sorted images from undersampled k-space data are being actively investigated.
Challenges: It is important to demonstrate that these methods which manipulate k-space maintain the fidelity of the image content and are able to faithfully reconstruct images. This requires close collaboration between developers of the techniques and the radiologists. Clinical studies are also required to demonstrate value of novel techniques and impact of these techniques on patient care.
Acknowledgements
No acknowledgement found.References
1. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, Kiefer B, Haase A. Generalized autocalibrating partially parallel acquisitions (GRAPPA) Magnetic resonance in medicine. 2002;47(6):1202–1210.
2. Sodickson DK, McKenzie CA. A generalized approach to parallel magnetic resonance imaging. Medical physics. 2001;28(8):1629–1643.
3. Lustig M, Donoho DL, Santos JM, Pauly JM. Compressed sensing MRI. IEEE Signal Proc Mag. 2008;25(2):72–82.
4. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine. 2014;72(3):707–717.
5. Zhang T, Cheng JY, Potnick AG, Barth RA, Alley MT, Uecker M, Lustig M, Pauly JM, Vasanawala SS. Fast pediatric 3D free-breathing abdominal dynamic contrast enhanced MRI with high spatiotemporal resolution. Journal of magnetic resonance imaging : JMRI. 2015;41(2):460–473.
6. Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. J Magn Reson Imaging. 2012 Jul;36(1):55-72.
Figures