5668
Hybrid 18F FDG PET/MRI in imaging cardiac sarcoidosis: a case based review.1Diagnostic Radiology/Nuclear Medicine and Molecular Imaging, University of Wisconsin School of Medicine and Public health, Madison, WI, United States, 2Internal Medicine/Cardiology, University of Wisconsin School of Medicine and Public health, Madison, WI, United States, 3Diagnostic Radiology/Cardiovascular imaging, University of Wisconsin School of Medicine and Public health, Madison, WI, United States
Synopsis
Early recognition of cardiac sarcoidosis (CS) is important to initiate early treatment and prevent heart failure and sudden cardiac death. However, diagnosis of CS can be challenging and requires a high-index of suspicion. Cardiac magnetic resonance imaging (CMR) and 18F-fluorodeoxyglucose PET (18F FDG PET) have opened new avenues in the detection of CS. Experience with hybrid PET/MRI at our institution demonstrates improved workflow, decreased patient radiation exposure (compared to PET/CT) and incremental diagnostic value in imaging of CS. Both modalities are complementary, and offer important diagnostic and prognostic clinical data.
Purpose
This is a case based review of the indications, protocols and utility of 18F FDG PET and MRI in diagnosis and management of cardiac sarcoidosis.Background
Incidence/Prevalence:
Cardiac sarcoidosis (CS) has been reported to involve 25%-76% of patients with systemic sarcoidosis, as revealed by autopsy and imaging studies. However most of CS is clinically silent with only about 5% of patients with systemic sarcoidosis are having symptoms of CS.1
Clinical manifestations:
The most common clinical manifestations of CS are conduction abnormalities, arrhythmias, congestive heart failure, and sudden cardiac death.1,2
Diagnosis:
Early recognition of subclinical disease is important to initiate treatment and prevent irreversible cardiac dysfunction and sudden cardiac death. However, CS can mimic other cardiomyopathies and diagnosis might be challenging due to nonspecific symptoms and low diagnostic yield of endomyocardial biopsy (EMB), electrocardiography, and conventional imaging.1,2
Two pathways to establish the diagnosis are defined. Histological diagnosis
from myocardial tissue can be used but has a diagnostic sensitivity of 20-30%
because of the patchy nature of the disease. Alternatively, histological proof
of extracardiac sarcoidosis can be combined with clinical features and cardiac
imaging for CS. Therefore, advanced imaging with cardiac magnetic resonance
(CMR) and positron emission tomography with
18F-fluorodeoxyglucose (18F FDG PET) have opened new avenues in the
detection of CS and evaluation of response to immunosuppressive treatment.1
Technique
Patient preparation:
Patient preparation prior to FDG administration is critical for achieving adequate suppression of physiological myocardial glucose uptake to visualize inflammation when normal myocardial cells use mainly free fatty acids (FFAs).1 Physiological FDG uptake can be reduced in normal myocardium by fasting, dietary modification, and intravenous administration of heparin.3 This exhibit will review specific details on patient preparation that ensure consistent, high-quality PET imaging.
Imaging:
Simultaneous and non-simultaneous 18 F FDG PET/MRI protocols will be presented with a focus on unique acquisition sequences for both approaches, including the need for specific sequences for MR attenuation correction, cardiac function and tissue characterization.
Findings
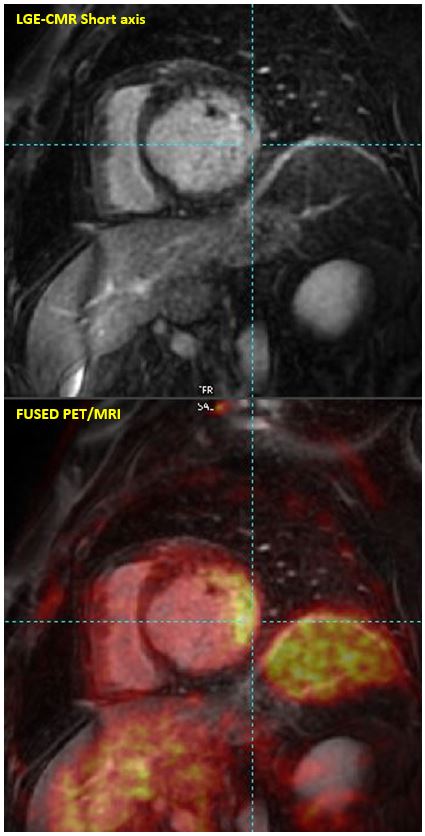
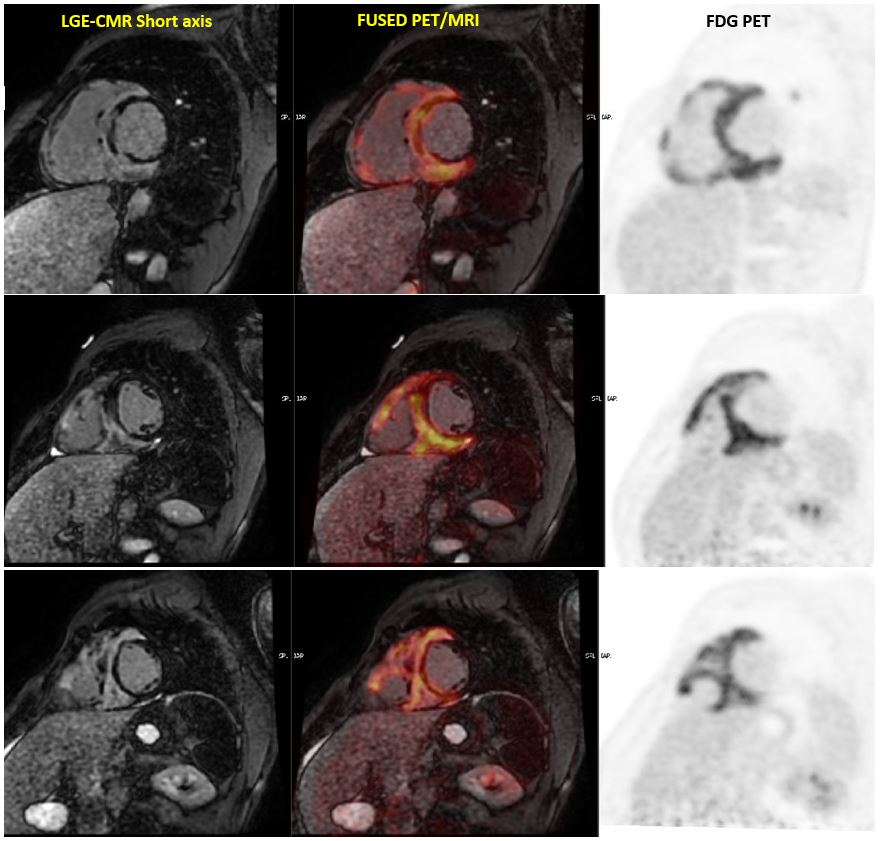
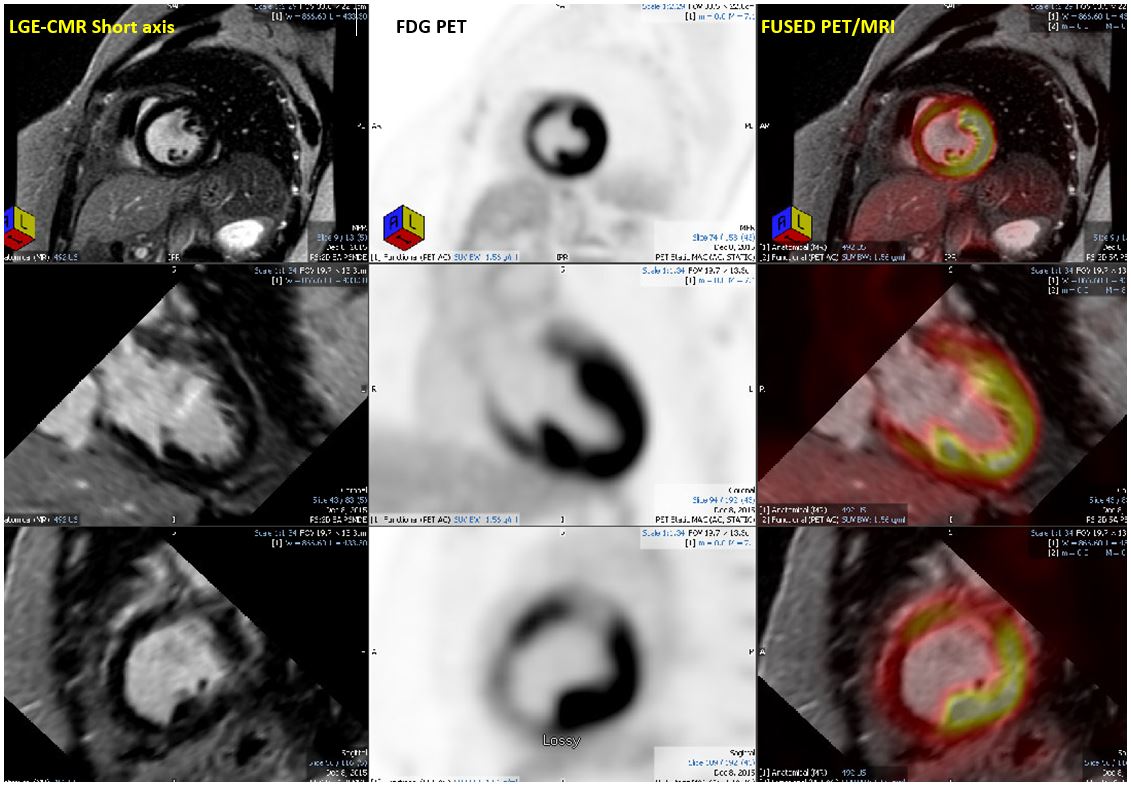
CMR findings of CS include focal areas of increased signal in late gadolinium enhancement (LGE) images, representing a combination of fibro granulomatous replacement and inflammation. Sarcoid lesions are often found in the midmyocardium and epicardium with a predilection for the basal and lateral segments of the left ventricle. T2-weighted CMR images depict edema as increased signal, suggestive of myocardial inflammation. However, sarcoid lesions can also be non-classic and located in the right ventricle free wall or present in an ischemic pattern with subendocardial or transmural lesions making the diagnosis even more challenging challenging.1 18 F FDG PET can serve an important role in these patterns of LGE.4
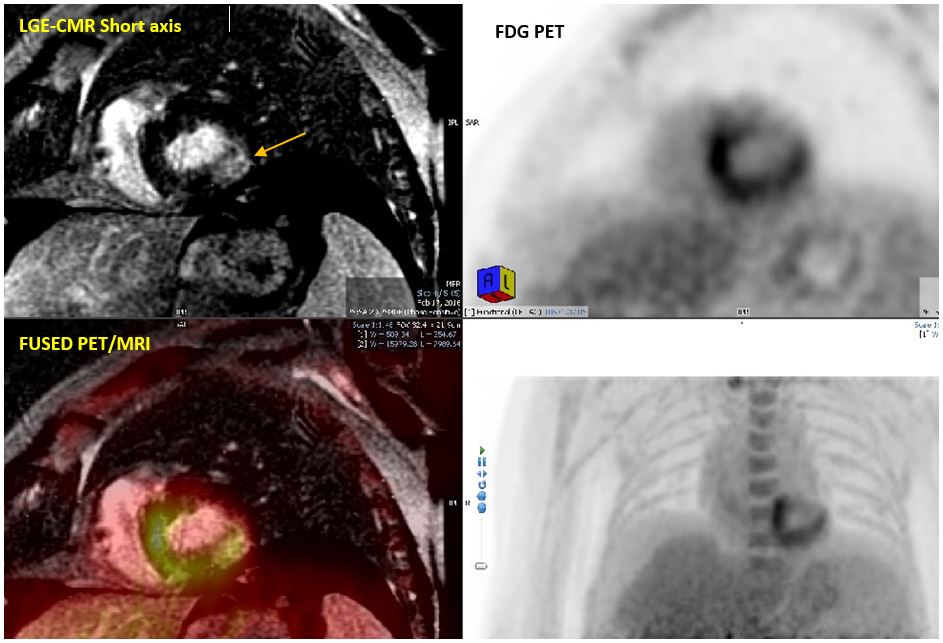
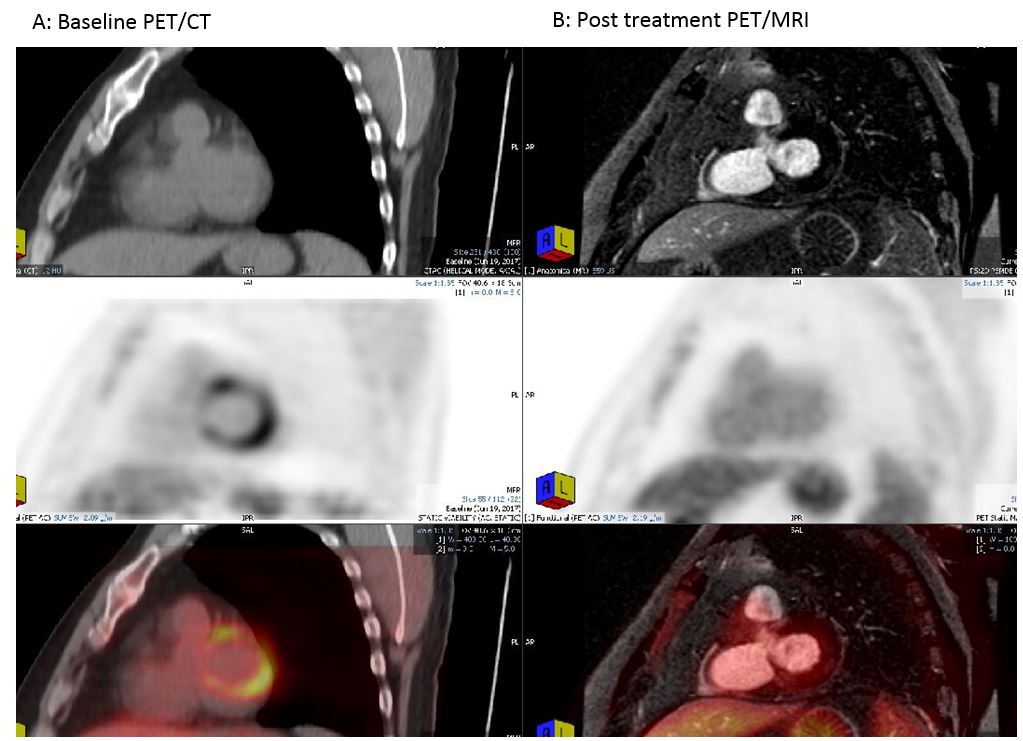
18 F FDG PET shows areas of hypermetabolic inflammatory activity within the myocardium corresponding to sarcoid lesions. Three typical patterns of FDG uptake are described: diffuse, focal, and focal on diffuse. CS is most typically associated with focal FDG uptake either in isolation or on a background of mild diffuse uptake. 5,6 Several studies have indicated that 18F FDG PET can also be used to monitor disease activity of CS during steroid therapy.4 In this review, we show 18 F FDG PET/MRI cases (either simultaneous or performed within a month interval) from our clinical experience to demonstrate the value of both modalities to accurately diagnose cardiac sarcoidosis. In some patients the CMRwas either nonspecific or negative while the PET showed focal FDG avidity suggestive of cardiac sarcoidosis. In other patients, the PET was negative or indeterminate for physiologic glucose metabolism versus sarcoidosis however CMR was suggestive of CS. For example, in figure 1, the distribution of LGE in the sub endocardium was nonspecific for scar from prior infarction versus CS. However, the PET showed focal FDG avidity corresponds to the area of delayed enhancement.
Summary
In conclusion, it is preferred to accommodate the work flow to perform 18 F FDG PET and CMR simultaneously when feasible for diagnosis of CS. The information from both modalities is typically complementary. In addition, simultaneous 18 F FDG PET/MRI will decrease patient radiation exposure compared to performing 18 F FDG PET/CT and MRI separately.Acknowledgements
NoneReferences
1. Anne L. Bakkera, Jan C. Gruttersb,c, Ruth G. Keijsersd, and Martijn C. Post. Cardiac sarcoidosis: challenges in clinical practice. Curr Opin Pulm Med. 2017 Sept;23(5):468-475.
2. Schindler TH. Emergence of Integrated Cardiac Magnetic Resonance/Positron Emission Tomography Imaging as the Preferred Imaging Modality in Cardiac Sarcoidosis. JACC Cardiovasc Imaging 2017 Jun 9. pii: S1936-878X(17)30451-5.
3. Hiroshi Ohira, Ichizo Tsujino, and Keiichiro Yoshinaga. 18F-Fluoro-2-deoxyglucose positron emission tomography in cardiac sarcoidosis.. Eur J Nucl Med Mol Imaging. 2011 Sep;38(9):1773-83.
4. Yamagishi H, Shirai N, Takagi M, Yoshiyama M, Akioka K, Takeuchi K, et al. Identification of cardiac sarcoidosis with (13)NNH(3)/(18)F-FDG PET. J Nucl Med 2003;44:1030–6.
5. Ishimaru S, Tsujino I, Takei T, Tsukamoto E, Sakaue S, Kamigaki M, et al. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates cardiac involvement of sarcoidosis. Eur Heart J 2005;26:1538–43.
6. Ohira H, Tsujino I, Ishimaru S, Oyama N, Takei T, Tsukamoto E, et al. Myocardial imaging with 18F-fluoro-2-deoxyglucose positron emission tomography and magnetic resonance imaging in sarcoidosis. Eur J Nucl Med Mol Imaging 2008;35:933–41.
Figures