5659
Fast Neuro MRI with Variable Refocusing Flip-Angle 2D SSFSE1Radiology, University of Wisconsin-Madison, Madison, WI, United States, 2Global MR Applications & Workflow, GE Healthcare, New York, NY, United States
Synopsis
A variable refocusing flip-angle method is described for 2D Single-Shot Fast Spin Echo (SSFSE) for fast imaging of the brain and spine, which can be beneficial in pediatric populations to avoid sedation and repeated CT exams. The scheme allows for full-Fourier k-space acquisitions with improved sharpness and T2 contrast, and faster imaging compared with conventional SSFSE.
Purpose
A variable refocusing flip-angle method is described for 2D Single-Shot Fast Spin Echo (2D-SSFSE) for fast imaging of the brain. This scheme allows for full-Fourier k-space acquisitions, shorter TR periods, improved sharpness and T2-contrast, and faster imaging compared with conventional SSFSE imaging.
Outline of Content
In conventional Fast Spin Echo (FSE) imaging, an RF excitation pulse is followed by a train of refocusing pulses (normally 130-160°) to acquire multiple lines of k-space per TR period. For very fast imaging, an entire plane of k-space data, with half-Fourier acquisition, can be acquired in a single-shot (HASTE or SSFSE), allowing a single slice of T2- or proton-density-weighted imaging in < 1s per slice. Such imaging methods have been used, for example, for fast exams that take <30s per series and <5 minutes table time in pediatric subjects as a motion-robust imaging method. This avoids the need for sedation or ionizing radiation exposure from repeated CT exams, for example, in monitoring shunt-treated hydrocephalus.1 The large number of RF refocusing pulses in conventional SSSFSE can limit acquisition speed based on T2-relaxation-based signal modulation and SAR restrictions, particularly at 3T and higher fields.
3D Fast Spin Echo (3D-FSE) has been used in neuroimaging, allowing reformatting in any plane. Such acquisitions are generally only practical with parallel imaging (e.g. GRAPPA, ARC) and variable refocusing flip angle schemes. The latter replace conventional refocusing pulses with a long train of lower flip angles, designed to extend the available magnetization for a much higher number of readout echoes.2 Recently, a variable refocusing flip angle scheme has been extended to 2D SSFSE for abdominal imaging (vrf-SSFSE), demonstrating increased imaging speed and improved image quality metrics compared with conventional SSFSE.3
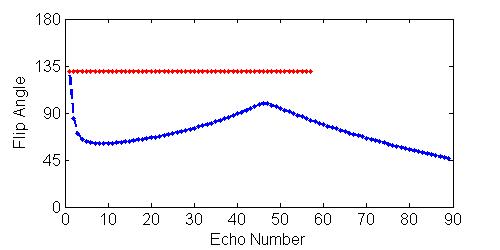
A similar technique can be applied for fast neuroimaging in pediatric populations.4 Figure 1 shows an example comparison of the flip angle scheme between a conventional SSFSE acquisition1 (red) and a similar acquisition with a variable refocusing flip-angle scheme3 (blue) at 3.0T for a 256x154 acquisition matrix. The conventional SSFSE acquisition used constant refocusing flip angles=130°; with TE=64ms and ETL=57 for a half-Fourier k-space acquisition. The vrf-SSFSE scheme used refocusing angles modulated by finit=130°, ftarget=60°, fcenter=100°, and fend=45°, with TEeff=102ms and ETL=89. The T2 prolongation effect due to the reduced flip angles allows full-Fourier acquisition at clinically-relevant TEs and phase resolution. Both schemes use ARC parallel imaging factor=2.
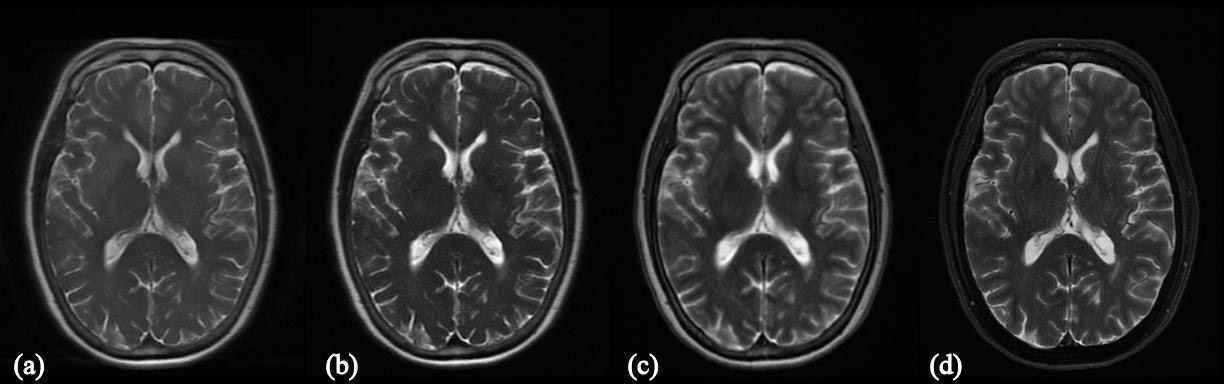
A comparison of the imaging methods is shown as an example in a normal subject at 3T (Figure 2). Images were acquired with a slice thickness of 5mm for comparison purposes. Shown are (Fig 2a) a conventional SSFSE sequence (TE=35ms); (2b) conventional SSFSE (TE=101ms); (2c) the variable refocusing flip SSFSE (TE=102ms); and, for comparison purposes, (2d) a conventional 2D FSE acquisition (TE=101ms). In addition to a much shorter scan duration for a full stack of 5mm slices (8s vs 29s), the vrf-SSFSE acquisition (2c) shows high T2 contrast compared with short-TE SSFSE (2a).
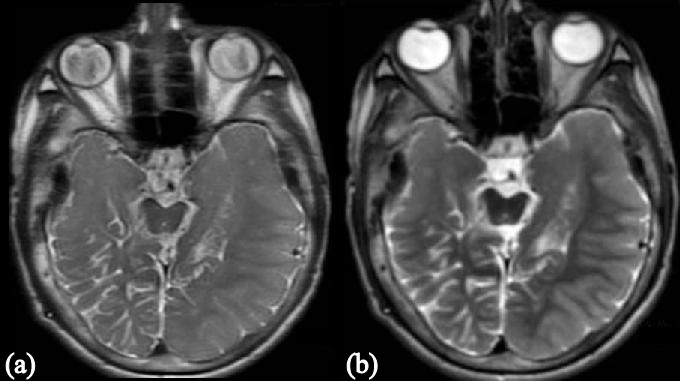
Figure 3 shows the application of the vrf-SSFSE method in a 13-year old patient with increasing seizures. (Fig 3a – Conventional SSFSE, TE=35ms; Fig 3b – vrf-SSFSE, TE=102ms).
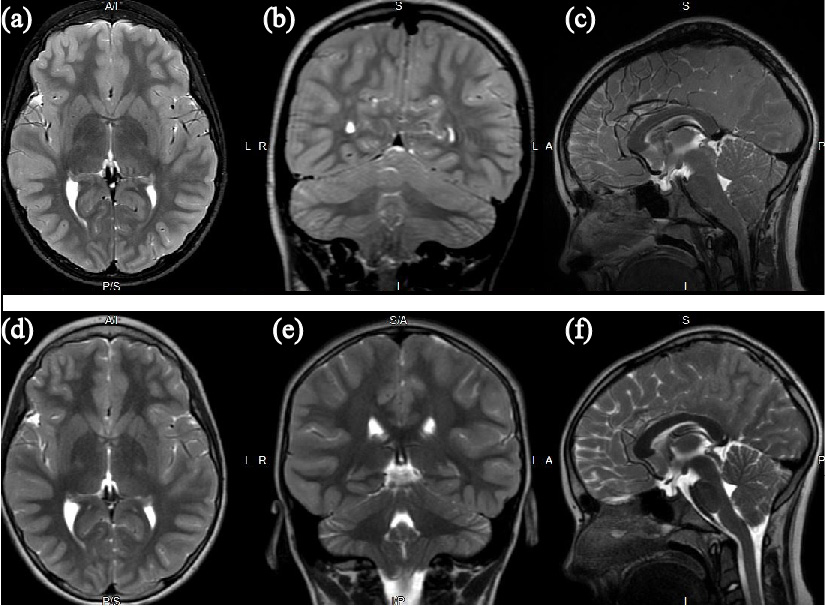
In Figure 4, the images from a conventional MRI exam are shown in comparison with 3 planes of the variable refocusing flip angle SSFSE in a 10-year old patient with Chiari I malformation. (4a: Ax T2 FSE; 4b: Cor-reformat T2-w CUBE; 4c: Sag T2-w CUBE; 4d-f: Ax, Cor, and Sag vrf-SSFSE).
Figure 5 shows images from axial, sagittal, and coronal vrf-SSFSE acquisitions in a pediatric patient, post-resection of a tectal plate astrocytoma, with hydrocephalus.
Summary
A variable refocusing flip-angle scheme has been described for 2D Single-Shot Fast Spin Echo (SSFSE) for fast imaging of the brain, which can be particularly beneficial in pediatric populations to avoid sedation and repeated CT exams. The scheme allows for full-Fourier k-space acquisitions with improved sharpness and T2 contrast, and faster imaging compared with conventional SSFSE.
Acknowledgements
No acknowledgement found.References
1. Iskandar BJ, Sansone JM, Medow J, and Rowley HA. The Use of Quick-Brain Magnetic Resonance Imaging in the Evaluation of Shunt-Treated Hydrocephalus. J Neurosurg Pediatrics 2004;101(2):147-151.
2. Busse RF, Brau A, Vu A, et al. Effects of Refocusing Flip Angle Modulation and View Ordering in 3D Fast Spin Echo. Magn Reson Med 2008;60:640–649.
3. Loening AM, Litwiller DV, Saranathan M, Vasanawala SS. Increased Speed and Image Quality for Pelvic Single-Shot Fast Spin-Echo Imaging with Variable Refocusing Flip Angles and Full-Fourier Acquisition. Radiology. 2017 Feb;282(2):561-568.
4. Darsie JC, Field AS, Rowley HA, et al. Increased Speed and Soft-Tissue Contrast in Single-Shot Fast Spin Echo Imaging Utilizing Tailored Refocusing Flip Angles for Fast Brain MRI. Proc. ASNR 55th Annual Meeting, Long Beach, CA, 2017: T-09.
Figures