5595
Thigh Muscle Recruitment Following Total Knee Replacement Surgery Using Dynamic Magnetic Resonance Elastography (DMRE)Michiel Robert Simons1,2, Michael Perrins2,3, Gwenllian Tawy4, Colin Brown5, Neil Roberts2, Edwin J.R. van Beek2, and Leela Biant4
1Department of Clinical Surgery, University of Edinburgh, Edinburgh, United Kingdom, 2Edinburgh Imaging Facility, University of Edinburgh, Edinburgh, United Kingdom, 3MRC Centre for Inflammation Research, University of Edinburgh, Edinburgh, United Kingdom, 4Department of Trauma & Orthopaedic Surgery, University of Manchester, Manchester, United Kingdom, 5The Mentholatum Company Ltd., East Kilbride, Glasgow, United Kingdom
Synopsis
In this study, Dynamic Magnetic Elastography (DMRE) is applied to a clinical cohort. DMRE scans were carried out in patients with severe OA pre and post-op Total Knee Replacement. Muscle recruitment was identified through increased muscle stiffness. Post operatively, muscle stiffness changes observed during dynamic loading were markedly less compared with their pre-op scan. This study supports the use of personalised targeted physiotherapy in muscle rehabilitation.
Introduction
The outcome of Total Knee Replacement (TKR) surgery is dependent on the accuracy of surgical implantation1. However, patient engagement with muscle rehabilitation plays a crucial role in achieving the best possible outcome2. Osteoarthritis (OA) is a joint deforming disease process which may lead to altered joint biomechanics3,4. This in turn can affect the mechanical properties and morphology of surrounding stabilizing musculature3,4,5. TKR can also result in acute injury to patients in surrounding tissue6. Bone marrow has been shown to impact on healing of patients, due to a limited release of nutrients to aid recovery7. To date there has been limited MRI studies investigating bone marrow, and never before using Magnetic Resonance Elastography, however imaging bone marrow can offer important clinical information with regards to patient health8. As part of this research, the newly developed method of using MRE, which we have named ‘Dynamic Magnetic Resonance Elastography’ (DMRE), will be implemented in order to investigate patient recovery. The aim of the study is to use DMRE in a clinical cohort in order to understanding static and dynamic changes in the mechanical properties of muscle tissue. It is hypothesised that there will be a reduced level of muscle strain in Quadriceps muscles following TKR due to the protective effects of post-op physiotherapy.Methods
Five TKR Patients (65.80[±10.38] years old) attended a Magnetic Resonance Elastography (MRE) scanning session pre-operatively and then 138.2(±51.20) days post TKR surgery. During the scanning session, axial MRE images were obtained initially at baseline where the knees were initially flexed at 50°, and subsequently partially extended to 25° during a knee extension which was sustained during image acquisition (80sec). MRE was performed with a Resoundant system which was attached through a non-inflated tourniquet cuff around the thigh of participants (Resoundant, Mayo Clinic, Rochester, MN, USA). Multi-frequency MRE9 (25, 37.5 and 50Hz) was obtained and processed with the ESP inversion algorithm10. Measuring mechanical properties at different levels of loading allows for a dynamic appreciation of muscle physiology, thus we have named our use of MRE as ‘Dynamic Magnetic Resonance Elastography’ (DMRE). Thigh elastograms were manually segmented for 12 individual muscles from four muscle groups including: Quadriceps muscle group (Rectus Femoris, Vastus Intermedius, Vastus Lateralis and Vastus Medialis) Hamstrings (Bicep Femoris [Long Head and Short Head], Semi-membranosus, and Semi-tendinosus), Adductors (Adductor Longus and Adductor Magnus), and also the Medial rotator muscles (Gracilis and Sartorius). Region of Interest (ROI) measurements were obtained for muscle stiffness (|G*| - kPa), between scanning session and changes in muscle |G*| during knee extension. Additional measurements were also obtained for muscle cross-sectional area (CSA - cm2) Changes were statistically analyzed through a Repeated Measures Multivariate ANOVA (MANOVA).Results
Muscle CSA had significantly decreased by 24% from the first scanning session compared to the second scanning session (106.45[±35.60]cm2 vs 80.72[±28.16]cm2). Elastograms showed that in the first scanning session a number of muscles were significantly strained during knee extension (Figure 1; Table 1) including Rectus Femoris (p=.006), Vastus Intermedius (p=.001), Vastus Lateralis p=.006), Vastus Medialis (p=.026) and Semi-membranosus (p=.020), as well as the thigh overall (p<.000). However, following TKR surgery overall muscle |G*| did not significantly increase during knee extension (p=.368). In addition to this, elastograms revealed that Rectus Femoris (p=.018), Vastus Lateralis (p=.010), and Sartorius (p=.030) all showed significantly greater muscle |G*| at baseline following surgery compared to the first scanning session. Bone marrow stiffness significantly increased in patients from the first scanning session compared to the time of the second scan (1.57[±.60] kPa vs 2.05[±.62], +31%, p=.046).Discussion
This research has highlighted that patients with severe OA awaiting TKR surgery in this cohort have weakened stabilising musculature. This is evident from the great increases in muscle stiffness observed with increased muscle loading. The aim of TKR is to restore this mechanical axis of the lower limb to regain stability and allow optimal muscle functioning. Post operatively the muscle stiffness changes observed with dynamic loading are significantly less. The 24% decrease in muscle size observed in the post op scanning session could be explained by muscle disuse atrophy secondary to surgical pain inhibition. There are significantly increased muscle stiffness changes observed in the hamstrings at baseline post operatively. These findings are supported by previous research as hamstrings are more prone to injury11.Conclusion
This is the first clinical study using DMRE to identify muscle recruitment around a TKR pre and post operatively. These findings support the use of a targeted physiotherapy approach to achieve best possible outcome following TKR surgery.Acknowledgements
No acknowledgement found.References
- Jeffery RS, Morris RW, Denham RA. Coronal alignment after total knee replacement. Bone & Joint Journal. 1991 Sep 1;73(5):709-14.
- Artz N, Elvers KT, Lowe CM, Sackley C, Jepson P, Beswick AD. Effectiveness of physiotherapy exercise following total knee replacement: systematic review and meta-analysis. BMC musculoskeletal disorders. 2015 Feb 7;16(1):15.
- Felson DT. An update on the pathogenesis and epidemiology of osteoarthritis. Radiologic Clinics. 2004 Jan 1;42(1):1-9.
- Felson DT. Osteoarthritis as a disease of mechanics. Osteoarthritis and cartilage. 2013 Jan 31;21(1):10-5.
- Hinman RS, Hunt MA, Creaby MW, Wrigley TV, McManus FJ, Bennell KL. Hip muscle weakness in individuals with medial knee osteoarthritis. Arthritis care & research. 2010 Aug 1;62(8):1190-3.
- Agung M, Ochi M, Yanada S, Adachi N, Izuta Y, Yamasaki T, Toda K. Mobilization of bone marrow-derived mesenchymal stem cells into the injured tissues after intraarticular injection and their contribution to tissue regeneration. Knee Surgery, Sports Traumatology, Arthroscopy. 2006 Dec 1;14(12):1307-14.
- Mankin HJ (1982) The response of articular cartilage to mechanical injury. J Bone Joint Surg Am 64:460–466
- Steinborn MM, Heuck AF, Tiling R, Bruegel M, Gauger L, Reiser MF. Whole-body bone marrow MRI in patients with metastatic disease to the skeletal system. Journal of computer assisted tomography. 1999 Jan 1;23(1):123-9.
- Papazoglou S, Rump J, Braun J, Sack I. Shear wave group velocity inversion in MR elastography of human skeletal muscle. Magnetic resonance in medicine. 2006 Sep 1;56(3):489-97.
- Barnhill E, Kennedy P, Johnson CL, Mada M, Roberts N. Real‐time 4D phase unwrapping applied to magnetic resonance elastography. Magnetic resonance in medicine. 2015 Jun 1;73(6):2321-31.
- Freckleton G, Pizzari T. Risk factors for hamstring muscle strain injury in sport: a systematic review and meta-analysis. Br J Sports Med. 2012 Jul 1:bjsports-2011.
Figures
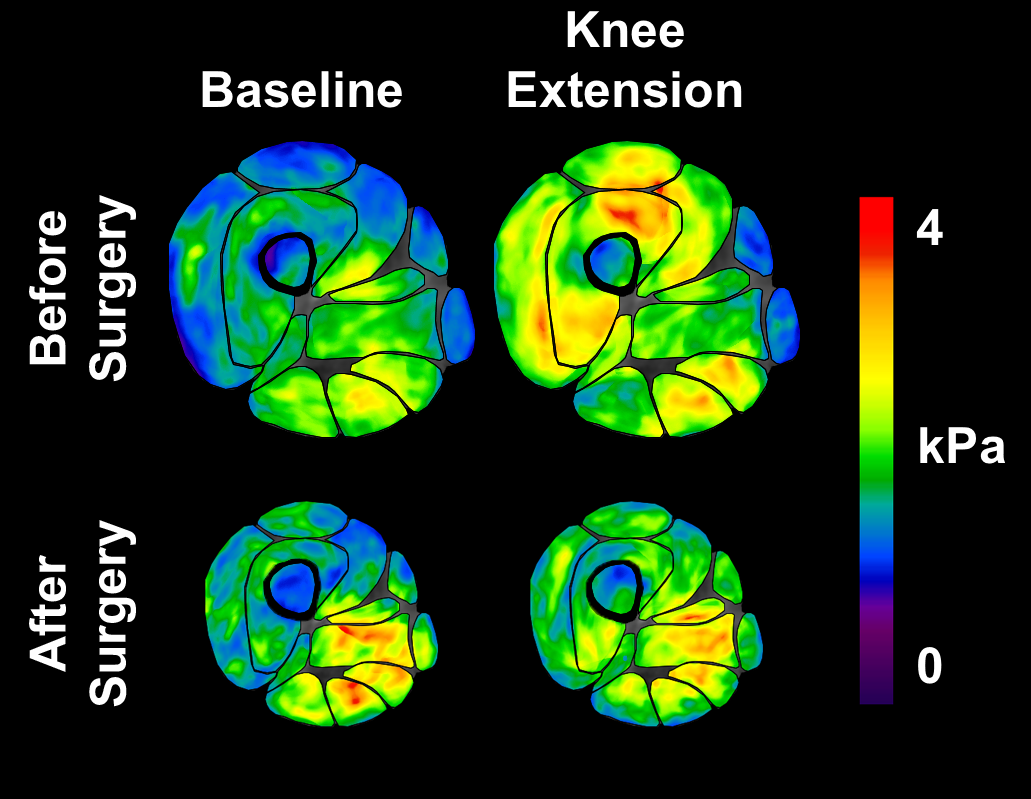
Figure 1 – Elastograms showing muscle |G*|
and morphology before and after TKR surgery
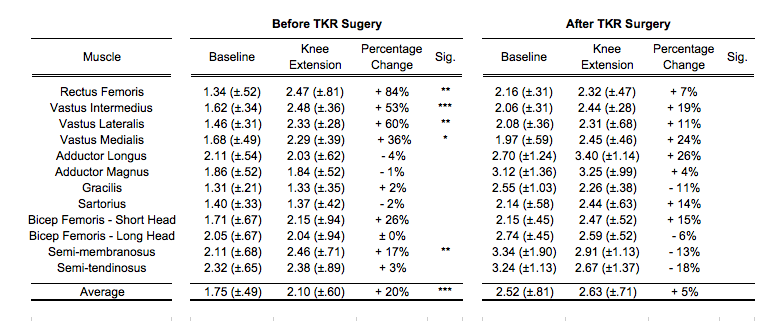
Table 1 – |G*| percentage changes during individual muscle
recruitment before and after TKR surgery
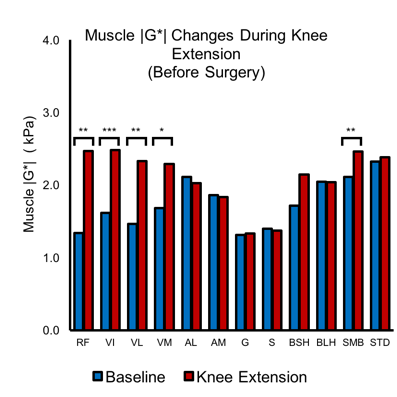
Figure 2 – Bar graph
showing mean muscle |G*| difference for individual muscle engagement before
surgery
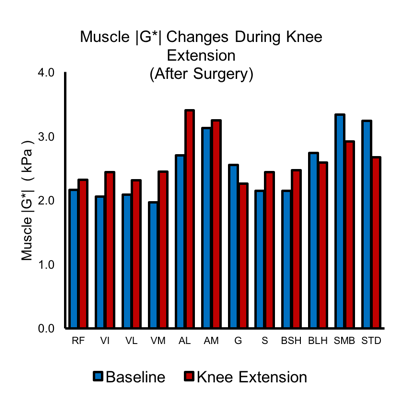
Figure 3 – Bar graph
showing mean muscle |G*| difference for individual muscle engagement after surgery