5594
Dynamic Magnetic Resonance Elastography (DMRE): A Novel Imaging Technique to Identify Active Muscle RecruitmentMichiel Robert Simons1,2, Michael Perrins2,3, Andre Attard4, Colin Brown5, Neil Roberts2, Edwin J.R. van Beek2, and Leela Biant6
1Department of Clinical Surgery, University of Edinburgh, Edinburgh, United Kingdom, 2Edinburgh Imaging Facility, University of Edinburgh, Edinburgh, United Kingdom, 3MRC Centre for Inflammation Research, University of Edinburgh, Edinburgh, United Kingdom, 4Dept of Bioengineering, University of Strathclyde, Glasgow, United Kingdom, 5The Mentholatum Company Ltd., East Kilbride, Glasgow, United Kingdom, 6Department of Trauma & Orthopaedic Surgery, University of Manchester, Manchester, United Kingdom
Synopsis
Dynamic Magnetic Resonance Elastography (DMRE) is a novel imaging technique which allows the quantification of muscle characteristics during a loaded MRE scan. Thigh muscle loading results in increased muscle stiffness. DMRE offers clinicians new insights into muscle engagement which aids in diagnosis and treatment for musculoskeletal pathologies. This work has shown DMRE is a sensitive tool to detect active muscle engagement.
Introduction
Increased muscle stiffness following muscle damage1,2, knee extension2,3, and muscle myopathies4 has been previously demonstrated using Magnetic Resonance Elastography (MRE), with recent muscle MRE research also being applied clinically to obtain new insight into muscle physiology5. Muscle stiffness changes from muscle loading could have important clinical applications in predicting peak muscle performance, and may aid in patient selection for surgery. In the present study, this is explored using MRE. Dynamic Magnetic Resonance Elastography (DMRE) has been developed to allow clinicians to assess morphometric muscle recruitment patterns allowing for a completely novel means of assessing tissue health. The aim of this current study is to investigate whether DMRE can identify muscle recruitment patterns and quantify changes in muscle strain from increased muscle loading. The hypothesis of this research is that the Quadriceps muscle stiffness will be primarily affected by increased loading.Methods
At baseline the knees of four participants (33.00[±9.06] years) were initially flexed at 50°, and subsequently partially extended to 25°. A custom designed muscle loading apparatus allowed for loading of the Quadriceps at increasing intervals (2kg, 4kg and 8kg) during concentric knee extensions. The loading equipment limited lower leg extension to 25°, which ensured participants extended consistently for each trial and enabled sustained steady loading during image acquisition (80sec). MRE was performed with a Resoundant system which was attached through a non-inflated tourniquet cuff around the thigh of participants (Resoundant, Mayo Clinic, Rochester, MN, USA). Multi-frequency MRE6 (25, 37.5 and 50Hz) was obtained of axial thigh slices and post-processed with the ESP inversion algorithm7. Measuring mechanical properties at different levels of strain allows for a dynamic appreciation of muscle physiology, with this technique being coined as ‘Dynamic Magnetic Resonance Elastography’ (DMRE). Thigh elastograms were manually segmented for 12 individual muscles from four muscle groups including: Quadriceps muscle group (Rectus Femoris, Vastus Intermedius, Vastus Lateralis and Vastus Medialis) Hamstrings (Bicep Femoris [Long Head and Short Head], Semi-membranosus, and Semi-tendinosus), Adductors (Adductor Longus and Adductor Magnus), and the Medial rotator muscles (Gracilis and Sartorius). DMRE was used to identified muscle recruitment through increased muscle stiffness (|G*|) from muscle loading. Groups were then formed based on muscles recruited (n=5) or non-recruited (n=7). Group averages were compared for muscle recruitment based |G*| changes. Region of Interest (ROI) measurements were obtained for muscle stiffness (|G*| - kPa), between groups, with changes being statistically analyzed through a repeated measures ANOVA.Results
The elastograms showed the recruitment pattern of thigh muscles during increased loading (Figure 1), the recruited muscle being the Quadriceps muscle group and Adductor Longus (Figure 2). There was no significant difference between the recruitment groups at baseline (p=.975), however recruited muscles |G*| significantly increased during loading (p<.000). Average recruited muscle |G*| increased from baseline (1.99[±.53] kPa) by 24% at 2kg (2.45[±.15] kPa; p=.099), by 28% at 4kg (2.54[±.15] kPa; p=.021), and by 45% at 8kg (2.87[±.15] kPa; p<.000; Figure 3), with no significant change in non-recruited muscles (p=.281). In the recruited muscles there was a significant correlation with load and |G*| (r[76]=.44, p<.000). Linear regression analysis showed that muscle |G*| was dependent on the load applied (R2=.19, F[1,78]=18.18, p<.000).Discussion
To our knowledge, this is the first study to show dynamic muscle recruitment using DMRE. This research has identified a co-contraction between Quadriceps and Adductor Longus. We determined that the Quadriceps generated force required for the task while the Adductor Longus contributed to knee extension stability. The finding in this study are in keeping with previous research showing that muscle stiffness is correlated with muscle use1,2,3,5. This work has shown that DMRE is a sensitive tool to detect muscle engagement with muscle loading. DMRE could be utilised in future research investigating muscle co-contraction in relation to injury, as this has been previously shown to be a major contributing factor2. The use of DMRE could help identify muscles at risk of injury and allow physiotherapists to employ personalised and targeted pre-habilitation and rehabilitation.Conclusion
DMRE has clear advantages over conventional imaging and has great potential to be used as a clinical tool. New insights into muscle engagement using DMRE offers clinicians new avenues for diagnosis and monitoring muscle health.Acknowledgements
No acknowledgement found.References
- Kennedy P, Macgregor LJ, Barnhill E, Johnson CL, Perrins M, Hunter A, Brown C, Beek EJ, Roberts N. MR elastography measurement of the effect of passive warmup prior to eccentric exercise on thigh muscle mechanical properties. Journal of Magnetic Resonance Imaging. 2017 Feb 1.
- Perrins M, Barnhill E, Braun J, Sack I, Hunter A, Brown C, van Beek EJR, Roberts N. Super-Resolution Magnetic Resonance Elastography (SR-MRE) of Exercise Induced Muscle Damage (EIMD). Proc. Intl. Soc. Magn. Reson. Med., (5981), 2016
- Barnhill E, Kennedy P, Hammer S, van Beek EJ, Brown C, Roberts N. Statistical mapping of the effect of knee extension on thigh muscle viscoelastic properties using magnetic resonance elastography. Physiological measurement. 2013 Nov 20;34(12):1675.
- Basford JR, Jenkyn TR, An KN, Ehman RL, Heers G, Kaufman KR. Evaluation of healthy and diseased muscle with magnetic resonance elastography. Archives of physical medicine and rehabilitation. 2002 Nov 30;83(11):1530-6.
- Perrins M, Hiscox L, Gray C, Semple S, Barclay L, Kirkbride R, Salisbury L, Brown C, Walsh T, van Beek EJR, Roberts N, Griffith D. Muscle Change Associated with Time in Intensive Care Unit (ICU). Proc. Intl. Soc. Magn. Reson. Med., (5069), 2017
- Papazoglou S, Rump J, Braun J, Sack I. Shear wave group velocity inversion in MR elastography of human skeletal muscle. Magnetic resonance in medicine. 2006 Sep 1;56(3):489-97.
- Barnhill E, Kennedy P, Johnson CL, Mada M, Roberts N. Real‐time 4D phase unwrapping applied to magnetic resonance elastography. Magnetic resonance in medicine. 2015 Jun 1;73(6):2321-31.
Figures
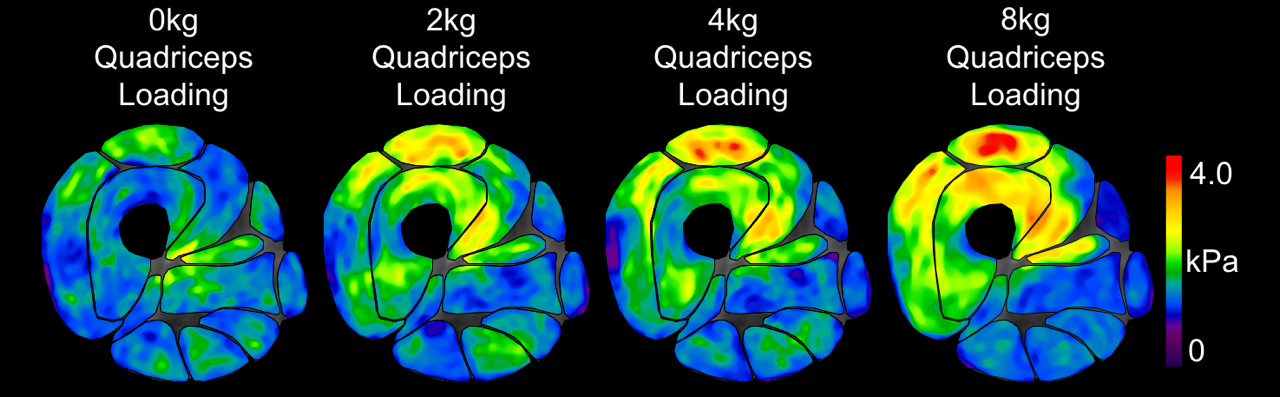
Figure 1. Graphical
visualisation of increased muscle |G*| during loading.
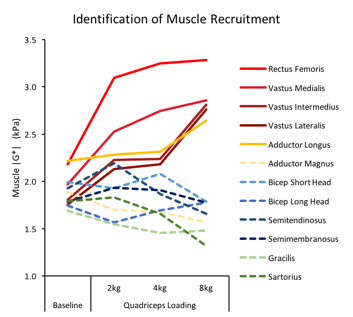
Figure 2.
Identification of recruited muscles by increasing muscle |G*|. Recruited
muscles shown as unbroken lines.
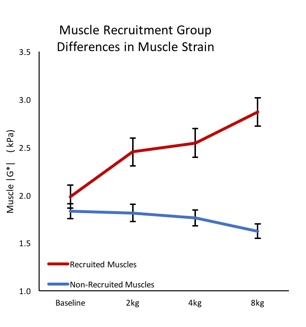
Figure 3. Muscle
recruitment group differences in muscle |G*| changes from loading.