5592
Magnetic Resonance Elastography (MRE) Reveals Muscle Instability in Middle Aged Healthy Adults1MRC Centre for Inflammation Research, University of Edinburgh, Edinburgh, United Kingdom, 2Edinburgh Imaging Facility, University of Edinburgh, Edinburgh, United Kingdom, 3Department of Clinical Surgery, University of Edinburgh, Edinburgh, United Kingdom, 4Department of Radiology, Icahn School of Medicine at Mount Sinai, Manhattan, NY, United States, 5Department of Physiotherapy, Queen Margaret University, Edinburgh, United Kingdom, 6The Mentholatum Company Ltd., East Kilbride, Glasgow, United Kingdom, 7Anaesthesia, Critical Care and Pain Medicine, University of Edinburgh, Edinburgh, United Kingdom
Synopsis
Age-related weakness and strength has been shown to have an anatomical basis, with stability of the knee being particularly prone to effects of ageing. Magnetic Resonance Elastography (MRE) was used to obtain muscle size and stiffness measurements in a ‘Younger’ and ‘Older’ group of participants. It was found that the Quadriceps muscle group were primarily impacted by age related atrophy, whilst also increasing in stiffness with age. Furthermore, the muscles along the medial side of the leg showed significantly lower muscle stiffness in ‘Older’ participants which we determined to be a biomarker for age-related anatomical instability.
Introduction
Age-related muscle atrophy primarily affects the Quadriceps muscle group when comparing 24 to 79 year olds1, with each of the four muscles within the Quadriceps shown to atrophy at the same rate. Age-related muscle atrophy of Vastus Lateralis has been suggested as an indicator for the whole quadriceps muscle group1, beginning at the age of 25, with atrophy then increasing incrementally with age2. Periods of immobility have been shown to be detrimental to muscle morphology3, however decreases in muscle size and strength seen in older individuals4 may be due to age-related changes in muscle fibres5,6. These changes result in gait instability7. Knee joint stability relies on static (joint congruency and ligaments) and dynamic stabilisers (surrounding musculature)8 with Quadriceps strength (determined by size4) and medial muscles playing a pivotal role9. Muscle recruitment patterns change with instability leading to increased co-contraction of antagonist muscles10. The purpose of the present study is to investigate age related changes to muscle morphology and mechanical properties, by applying Magnetic Resonance Elastography (MRE) to identify changes in the mechanical properties of middle aged adults’ thigh muscles for biomarkers of gait instability. The hypothesis of this study is that the Quadriceps will be primarily affected by age related atrophy, and biomarkers for age related instability will occur down the medial side of the thigh.Methods
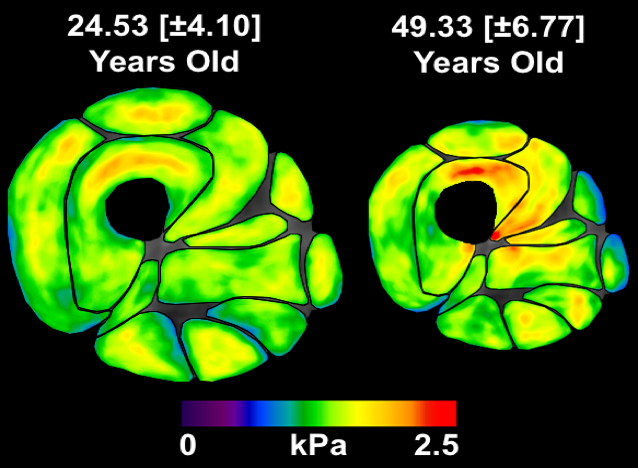
Participants were grouped into two groups depending on age, with a ‘Younger’ group (24.53[±4.10] years old, n=15) and an ‘Older’ group (49.33[±6.77] years old, n=6). Multi-frequency MRE11 was carried out (25, 37.5, 50, 62.5Hz) followed by ESP post-processing12. Thighs were manually segmented into 12 individual muscles of four muscle groups: Quadriceps (Rectus Femoris, Vastus Lateralis, Vastus Intermedius and Vastus Medialis), Hamstrings (Biceps Femoris Long Head, Bicep Femoris Short Head, Semimembranosus and Semitendinosus), Adductors (Adductor Magnus and Adductor Longus) and the Medial rotator muscles (Gracilis and Sartorius). Region of interest (ROI) analysis was performed for cross-sectional area (CSA - cm2) and muscle stiffness (|G*| - kPa), across ages (20-55 years old) and also between the two age groups. Multivariate ANOVA (MANOVA) was used to analyse ROI measurements between age groups.Results
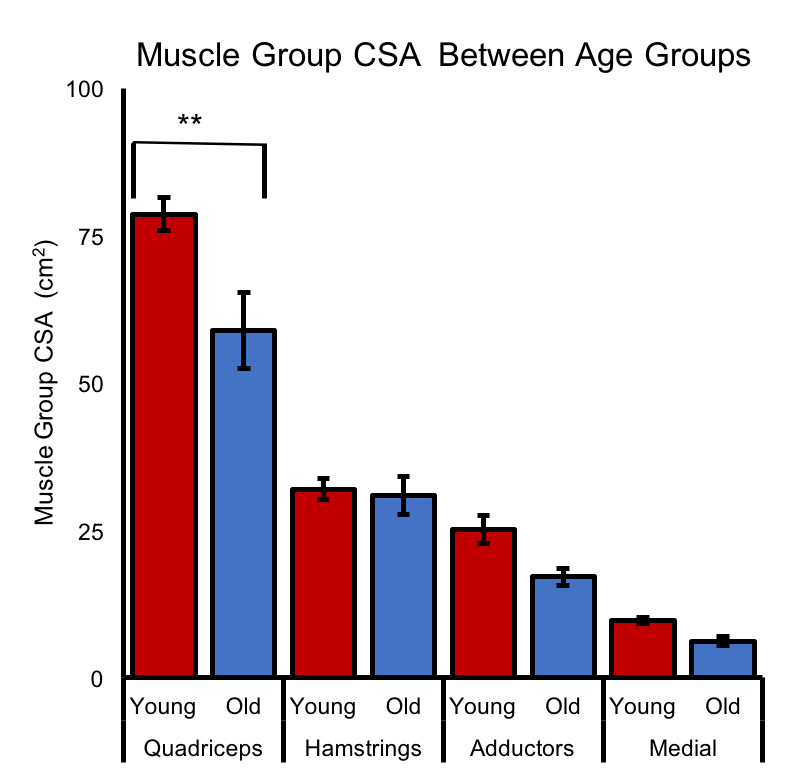
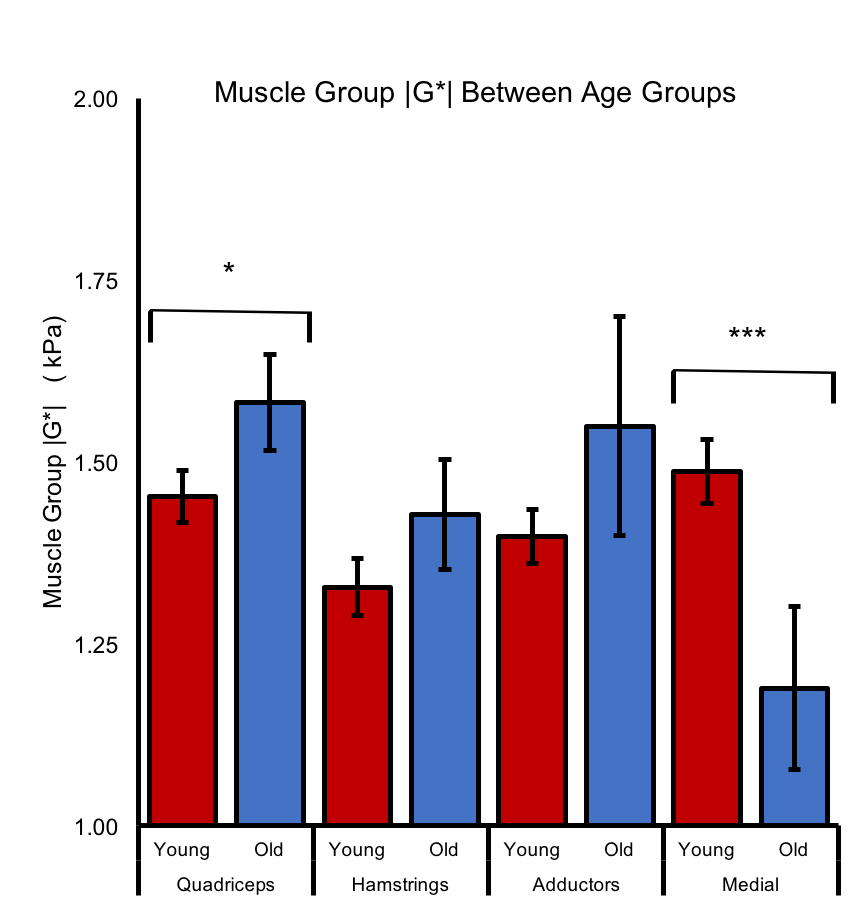
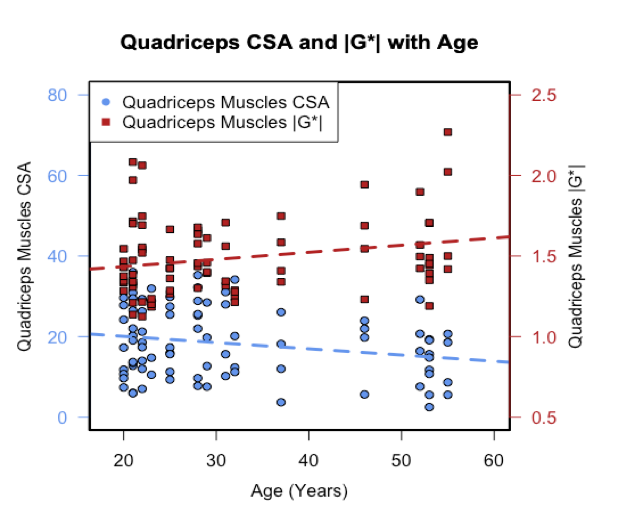
Overall thigh CSA was 22% lower in the ‘Older’ group (Figure 1) compared to the ‘Younger’ group (p=.008). The Quadriceps were primarily affected by ageing, with the ‘Older’ group showing a 25% decrease in Quadriceps CSA compared to the ‘Younger’ group (p<.000), particularly in the Vastus Lateralis (-33%; p=.004) There were no significant differences between age groups in CSA (Figure 2) for the Hamstrings (p=.999), Adductors (p=.489) and Medial muscles (p=.988). |G*| was significantly greater in the ‘Older’ group compared to the ‘Younger’ group for the Quadriceps (+9%; p=.021; Figure 3). There was a significant correlation for age (Figure 4) with Quadriceps CSA (r[82]=-.22; p=.049) and |G*| (r[82]=.23; p=.033). Finally, |G*| was significantly lower in the Medial muscles of the ‘Older’ group than the ‘Younger’ group (1.19[±.30] kPa vs 1.49[±.20] kPa; -20%; p=.001), with a significant negative correlation co-efficient for this decrease across ages (r[40]=-.50; p=.001). Linear regression analysis showed that age had a significant effect on Medial muscle |G*| (R2=.25, F[1,40]=13.08, p<.000).Discussion
The findings of the present study support previous research which found that the Quadriceps were primarily effected by ageing-effects1. The quadriceps muscle did not atrophy uniformly with the greatest decrease observed in Vastus Lateralis. Interestingly, muscle stiffness of the Quadriceps increased with age, while muscle stiffness of the Medial muscles decreased. Muscle MRE has been sensitive to muscle stiffness change with age and has identified two potential signs of age related mechanical weakness. Firstly, decreased Quadriceps muscle group size as this is an anatomical basis for muscle strength4. Secondly, the reduction in the medial muscles stiffness could be seen as an early biomarker for age related instability, since previous research has shown the importance muscle co-activation10, particularly for the medial muscles9. The results shown here suggest that the medial muscles would be considerably less stable in supporting the ‘Older’ group compared to the ‘Younger’ group.Conclusion
We conclude that through the use of MRE we demonstrated evidence for detection of age related weakness and anatomical instability in middle ages adults, due to morphometric and mechanical changes in thigh muscle.Acknowledgements
No acknowledgement found.References
1. Trappe TA, Lindquist DM, Carrithers JA. Muscle-specific atrophy of the quadriceps femoris with aging. Journal of Applied Physiology. 2001 Jun 1;90(6):2070-4.
2. Lexell J, Taylor CC, Sjöström M. What is the cause of the ageing atrophy?: Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15-to 83-year-old men. Journal of the neurological sciences. 1988 Apr 30;84(2):275-94.
3. Perrins M, Hiscox L, Gray C, Semple S, Barclay L, Kirkbride R, Salisbury L, Brown C, Walsh T, van Beek EJR, Roberts N, Griffith D. Muscle Change Associated with Time in Intensive Care Unit (ICU). Proc. Intl. Soc. Magn. Reson. Med., (5069), 2017
4. Frontera WR, Hughes VA, Fielding RA, Fiatarone MA, Evans WJ, Roubenoff R. Aging of skeletal muscle: a 12-yr longitudinal study. Journal of applied physiology. 2000 Apr 1;88(4):1321-6.
5. Faulkner JA, Brooks SV, Zerba E. Muscle atrophy and weakness with aging: contraction-induced injury as an underlying mechanism. The journals of gerontology. Series A, Biological sciences and medical sciences. 1995 Nov;50:124-9.
6. Evans WJ, Lexell J. Human aging, muscle mass, and fiber type composition. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 1995 Nov 1;50(Special Issue):11-6.
7. Kang HG, Dingwell JB. Effects of walking speed, strength and range of motion on gait stability in healthy older adults. Journal of biomechanics. 2008 Oct 20;41(14):2899-905.
8. Schipplein OD, Andriacchi TP. Interaction between active and passive knee stabilizers during level walking. Journal of Orthopaedic Research. 1991 Jan 1;9(1):113-9.
9. Warren LF, Marshall JL, Girgis F. The prime static stabilizer of the medial side of the knee. JBJS. 1974 Jun 1;56(4):665-74.
10. Schmitt LC, Rudolph KS. Influences on knee movement strategies during walking in persons with medial knee osteoarthritis. Arthritis Care & Research. 2007 Aug 15;57(6):1018-26.
11. Papazoglou S, Rump J, Braun J, Sack I. Shear wave group velocity inversion in MR elastography of human skeletal muscle. Magnetic resonance in medicine. 2006 Sep 1;56(3):489-97.
12. Barnhill E, Kennedy P, Johnson CL, Mada M, Roberts N. Real‐time 4D phase unwrapping applied to magnetic resonance elastography. Magnetic resonance in medicine. 2015 Jun 1;73(6):2321-31.
Figures