5578
BOLD activation pattern of cerebrum for unilateral and bilateral wrist extension task among stroke patients and healthy subjects1Centre for Biomedical Engineering, Indian Institute of Technology Delhi, New Delhi, India, 2Department of Biomedical Engineering, All India Institute of Medical Sciences, NEw Delhi, India, 3Department of Psychiatry, All India Institute of Medical Sciences, NEw Delhi, India, 4Department of Neurology, All India Institute of Medical Sciences, NEw Delhi, India, 5Department of Nuclear Magnetic Resonance, All India Institute of Medical Sciences, NEw Delhi, India
Synopsis
Role of wrist-extension in motor control in upper-limb post-stroke recovery is significant. We compared neural structures controlling unilateral versus bilateral movement of wrist-extension task using fMRI in 6 healthy-volunteers and 6 stroke-patients. Significant BOLD activation was observed in PG during all three tasks in healthy-volunteers. Activation with bilateral-task were considerably higher than unilateral-task. In patients with stroke as a result of re-organization, ipsi-lesion cerebellum-area shows activation for affected-hand movement not present in healthy-volunteers, supporting evidence for advantages of bilateral-training in functional imaging. Knowledge of reorganization-pattern for coordinated-movement involved in bilateral-tasks may be helpful in addressing the rehabilitation of stroke-patients.
Purpose:
The evidence that extra neural-activity during coordination of bilateral movement could result in neuroplasticity [1] encouraged us to study the additional neural-activity in bilateral-coordination and differences in activation-pattern of unilateral and bilateral movement of complex-task in stroke-patients and healthy-volunteers. Despite considerable progress made towards neural control of simple and complex finger-tasks movements and its coordination, neural basis of coordination of wrist-extension task playing significant role in stroke recovery still remains largely unresolved because of the complexity of the joint and larger muscles involvement. In order to develop an evidence-based post-stroke rehabilitation protocols, we attempted to evaluate activation differences between healthy-volunteers and stroke-patients for complex-task.Methods:
Experiment: 6 healthy and 6 patients with right-MCA stroke (within 2 years of chronicity), all right-handed subjects (M:F=4:2,Age=21-30Yrs) were scanned while they performed three self-paced consecutive wrist-extension tasks in full range of motion– Left-hand only (LH), Right-hand only (RH) and both-hand simultaneously (BH) while lying in supine position with palms facing downwards. The tasks consisted of 3 sessions-LH, RH and BH of 6 minutes each using block design paradigm of 40 seconds active and rest state each (4 cycles) with a total of 180 dynamics.
Data acquisition, Pre-processing and Analysis: 3T MR scanner (Achieva 3T TX, M/s. Philips Healthcare) with 31 ascending transversal slices, was used for acquiring the data with TR=2000 ms, FOV= 230x230x155 mm, Flip angle: 900, voxel-size:1.8x1.8x5 mm, TE=30 ms. For healthy-volunteers data was acquired twice with a gap of 8-14 weeks for robustness. Slice time correction, realignment, normalization, smoothing with 8x8x8 FWHM were performed to pre-process the fMRI data. General Linear Model was employed to evaluate intra-subject contrast maps and for second level analysis one sample t-test threshold p<0.01 (FDR corrected) at minimum 15 voxels per cluster was performed to evaluate the activation during each task. Paired t-test (p<0.001 uncorr., minimum 15 voxels per cluster) was used for between-task comparison. Automated Anatomical Labeling (AAL) was used to label the activated brain areas of each cluster. For each cluster-activation maximum of three peaks of activation are shown.
Results:
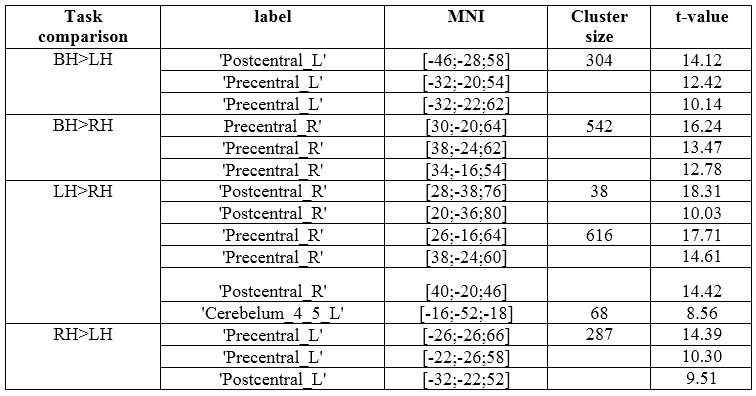
Healthy: Peak-activation were observed in respective Contralateral (CL) Precentral Gyrus (PG) during all 3 individual-tasks (LH, RH & BH) (table 1). Comparison of peak-activation for bilateral vs unilateral and left hand vs right hand is shown in figure 1&2. Highest activated cluster in LH was in CL PG, Ipsialteral (IL) and CL Supplementary motor area (SMA) and IL cerebellar-areas along with few subcortical activations. RH shows focused activation only in CL PG and SMA and no activation IL and CL cerebellar-areas (table 1, figure 2). BH shows activation in both, left and right PG, SMA, cerebellar-areas along with few sub-cortical areas. BH>LH shows activation in Postcentral Gyrus left (PoG_L) with cluster spread to PG_L and BH>RH reveals activation focused in PG_R. Both LH>BH and RH>BH did not show any significant activation indicating no extra activation associated during unilateral movement.
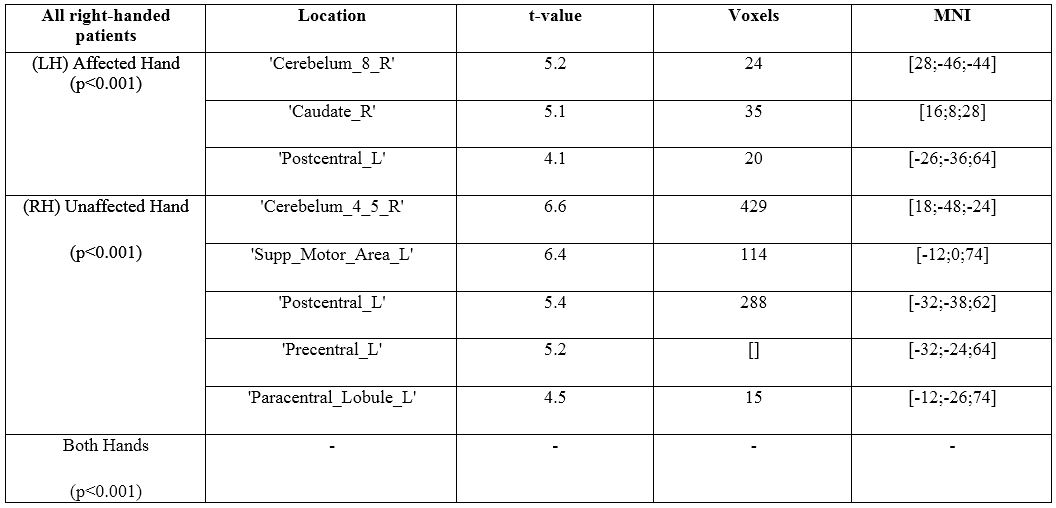
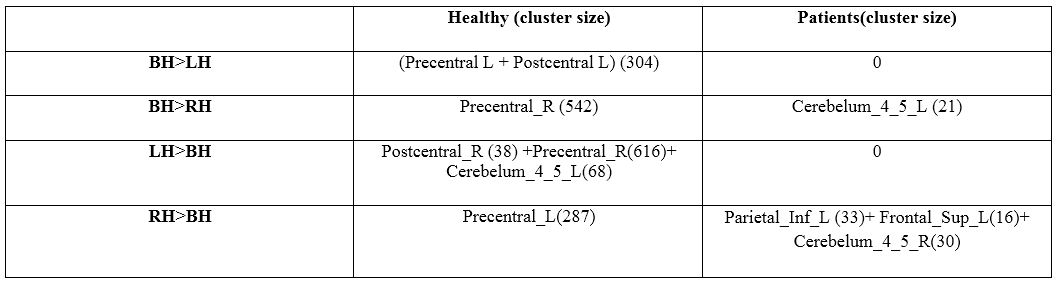
Patients: In case of both affected and unaffected-hand, right cerebellum shows activation (table 2). When unilateral-tasks (RH and LH) were compared with bilateral-task (BH) (table 3) BH did not exhibit any significant activation compared with affected-hand(LH) and unaffected-hand(RH) at p<0.001. BH>RH showed activation in cerebellum-areas but RH>BH showed activation in left parietal-area spreading to left PoG along with activation in left frontal (non-motor region) and right cerebellum-regions(table 2).LH>BH and BH>LH showed no activation left-hand being the affected hand in patients (table 3).
Discussion:
The present findings indicate that sequential wrist-extension of individual limbs does not show any additional motor activation as activated in bilateral limbs [2]. The involvement of SMA in bilateral-coordination observed in our study is consistent with literature [3]. Voxel-wise activation showed greater sub-cortical (insula, putamen and thalamus) and cerebellum-areas during BH as compared to RH and LH alone. This supports that several motor regions with higher activation in the bilateral-condition than unilateral-conditions which might be due to Inter Hemispheric Inhibition, given that region mutually inhibits each other thus requiring greater activity to overcome inhibitory signals and cross threshold to move the limb, and as well as from greater need for motor coordination [4]. The analysis also highlighted differential role for left and right hemispheres during BH movements, further elaborating concept of handedness. Comparison of healthy and patients BH>RH and RH>BH highlights reorganization of ipsi-lesion cerebellum-area (right) in patients. This shows that ipsi-leisional cerebellum plays an important role in reorganization in motor task after stroke. Therefore, unaffected-hand training can play role in ipsileisional reorganization supporting the hypothesis & advantage of bilateral training over unilateral training.Acknowledgements
Authors would like to thanks SERB, Department of Science and Technology, Govt. of India for providing financial support for this project, project number YSS/2015/000697.References
[1] J. Whitall, S. M. Waller, J. D. Sorkin, L. W. Forrester, R. F. Macko, D. F. Hanley, A. P. Goldberg, and A. Luft, “Bilateral and unilateral arm training improve motor function through differing neuroplastic mechanisms: a single-blinded randomized controlled trial.,” Neurorehabil. Neural Repair, vol. 25, no. 2, pp. 118–29, Feb. 2011. [2] C. Horenstein, M. J. Lowe, K. A. Koenig, and M. D. Phillips, “Comparison of unilateral and bilateral complex finger tapping-related activation in premotor and primary motor cortex,” Hum. Brain Mapp., vol. 30, no. 4, pp. 1397–1412, Apr. 2009. [3] L. Jäncke, M. Peters, M. Himmelbach, T. Nösselt, J. Shah, and H. Steinmetz, “fMRI study of bimanual coordination.,” Neuropsychologia, vol. 38, no. 2, pp. 164–74, 2000. [4] J. W. Noble, J. J. Eng, and L. A. Boyd, “Bilateral motor tasks involve more brain regions and higher neural activation than unilateral tasks: An fMRI study,” Exp. Brain Res., vol. 232, no. 9, pp. 2785–2795, 2014.Figures