5570
Brain response to stop signal task in lifelong Premature Ejaculation patients compared to healthy subjects1Engineering Research Center of Molecular and Neuro Imaging of the Ministry of Education, School of Life Science and Technology, Xidian University, Xi’an, Shaan xi, China, 2Department of Urology, Xijing Hospital, The Fourth Military Medical University, Xi’an, Shaanxi, China, 3The ART Center, Maternal and Child Health Care Hospital of Shaanxi Province, Xi’an, China
Synopsis
Life-long premature ejaculation (LPE) is a common male sexual dysfunction. Previous studies revealed ejaculation-related control mechanisms in the brain. However, whether this control network changes in patients with LPE is unclear. A stop signal test was used in this study. A study of task-related functional MRI found there was a significant difference in neural network activation between healthy controls and LPE patients during go process. This study indicates a neural network abnormality in LPE patients, which provides novel reference for understanding the neural mechanism of LPE.
Introduction
Lifelong premature ejaculation (LPE) is characterized by ejaculation that always or nearly always occurs prior to or within about one minute of vaginal penetration since the first sexual experience. Up to now, the central neural mechanism of LPE remains unclear. In this year, several neural imaging studies have shown abnormalities in cerebral function and structure in LPE patients by the first time. It suggests an underlying role of high brain centers being involved in the biological mechanism of LPE. Moreover, consideration of the behavioral features of LPE, e.g. disability on suppression of imminent ejaculation behavior, it is similar to some diseases with inhibitory deficits. Therefore, it is interesting to know whether the brain control network was damaged in LPE patients. The stop signal task (SST) is a classical experimental task to detect human control ability and neural correlates. Thus, we compared the neural activation respond to SST between LPE patients and healthy controls in order to investigate the possible functional changes of central control network in LPE patients.Methods
Twenty healthy controls (31.23±4.07) and 25 LPE patients (31.88±4.33) were recruited. All participants were heterosexual right-handed male Chinese volunteers. LPE diagnoses were based on the International Society for Sexual Medicine guidelines and DSM-5™. Patients did not receive any treatment at least 2 weeks before experiment. There was no differences in intelligence quotient between groups. Intravaginal ejaculatory latency time (IELT) and premature ejaculation diagnostic tool (PEDT) score was significantly different between the healthy controls (IELT: 6.55±3.87; PEDT: 0.60±1.13) and LPE patients (IELT: 0.36±0.17; PEDT: 17.58±1.78) (p < 0.0001). Written informed consent was obtained from all study participants. Research procedures were conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
The SST used in the present study was similar to that reported. We used the quantile method to determine SSTR. The task-related functional magnetic resonance imaging data were collected using a 3T MRI system (EXCITE, General Electric, Milwaukee, WC, USA) at a local hospital. We used SPM12 (http://www.fil.ion.ucl.ac.uk/spm) and the MATLAB 2012a software package (MathWorks, Natick, MA, USA) to process fMRI data. The following events were modeled after a Standard general linear model: successful go (Go), successful inhibit (StopInhibit), failure inhibit (StopRespond). Empty events were not explicitly modelled, and thus constituted an implicit baseline. For each subject and each scan, calculated the following six contrasts: Go-null, StopInhibit-null, StopRespond-null, StopInhibit-Go, StopInhibit-StopRespond and StopRespond-Go. The active regions of the six contrasts in LPE patients and healthy controls were analyzed at the whole brain level using a one sample t-test. Age was included as a covariate (FWE, p < 0.05). Using a two sample t-test, we calculated the difference in brain activation of the six contrasts between healthy controls and LPE patients at the whole brain level. Age was included as a covariate (p < 0.001 uncorrected and cluster size p < 0.05 FDR corrected).
Results
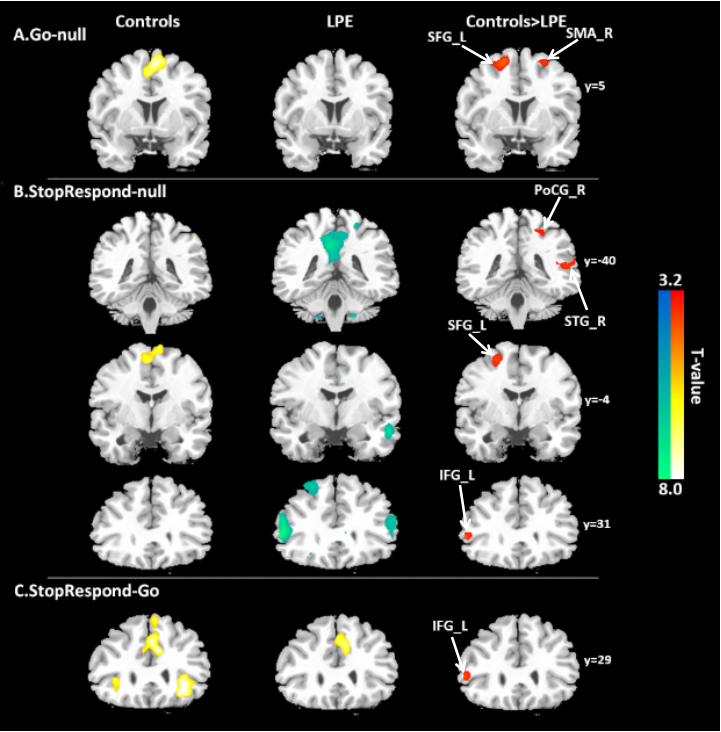
In the contrast of Go-null, healthy controls showed significantly enhanced in left superior frontal gyrus (BA6, SFG_L) and right supplementary motor area (BA6, SMA_R) compared with LPE patients (Figure 1A). And in the contrast of StopRespond-null, stronger activation in healthy controls was observed in right postcentral gyrus (BA3, PoCG_R), right superior temporal gyrus (BA42, STG_R), left superior frontal gyrus (BA6, SFG_L) and left inferior frontal gyrus (BA45, IFG_L) than LPE patients (Figure 1B). In the contrast of StopRespond-Go, compared with LPE patients, healthy controls showed significantly increased activation in IFG_L (Figure 1C).
During three stop process-related activations, there was no difference between the healthy controls and the LPE patients.In the contrast of StopInhibit-null, the right medial frontal cortex, SMA, anterior cingulate cortex, parietal cortex, and insula cortex were activated both in healthy controls and LPE patients. In the contrast of StopInhibit-Go which directly reflects the brain inhibitory response, the right IFC, right pre-SMA, in addition to other regions such as right parietal cortex and right insula were activated in two groups which were similar to previous studies. Finally, we also contrasted StopInhibit-StopRespond. The activation patterns included of bilateral Inferior occipital gyrus in two groups. In LPE patients, bilateral activation in putamen was also observed. But there was no significant difference between groups.
Conclusions
In this study, we found abnormalities of neural network activation in LPE patients during go process. Although we currently didn’t find significant differences between healthy controls and LPE patients in stop-related neural activation . Interaction analysis of corrrelations between SST performance and neural activations is worthy of studying in the future, for further detecting the central inhibitrory network of LPE patients.Acknowledgements
No acknowledgement found.References
Aron AR, Poldrack RA. Cortical and subcortical contributions to Stop signal response inhibition: role of the subthalamic nucleus. J Neurosci. 2006;26(9): 2424-2433.
Band GP, van der Molen MW, Logan GD. Horse-race model simulations of the stop-signal procedure. Acta Psychol (Amst). 2003;112(2): 105-142.
Bing Zhang. Functional insights into aberrant brain responses and integration in patients with lifelong premature ejaculation. August 19, 2016. www.nature.com. accessed February 21,2017.
Bonnelle V, Ham TE, Leech R, Kinnunen KM, Mehta MA, Greenwood RJ, et al. Salience network integrity predicts default mode network function after traumatic brain injury. Proc Natl Acad Sci USA. 2012;109(12): 4690-4695.
Galvan A, Poldrack RA, Baker CM, McGlennen KM, London ED. Neural correlates of response inhibition and cigarette smoking in late adolescence. Neuropsychopharmacology. 2011;36(5): 970-978.
Logan GD. On the ability to inhibit thought and action: A users' guide to the stop signal paradigm. Inhibitory processes in attention, memory, and language. 1994: 189-239. San Diego: Academic Press.
Van Rooij D, Hoekstra PJ, Mennes M, von Rhein D, Thissen AJ, Heslenfeld D, et al. Distinguishing Adolescents With ADHD From Their Unaffected Siblings and Healthy Comparison Subjects by Neural Activation Patterns During Response Inhibition. Am J Psychiatry. 2015a;172(7): 674-683.
Figures