5542
Functional Connectivity-Based Classification of Gulf War Illness Patients vs Control Veterans1Computer Engineering, University of Houston - Clear Lake, Houston, TX, United States, 2VA RR&D Center of Excellence, Atlanta VAMC, Decatur, GA, United States, 3Neurology, Emory University, Atlanta, GA, United States, 4Internal Medicine, UT Southwestern Medical Center, Dallas, TX, United States, 5Radiology, Emory University, Atlanta, GA, United States
Synopsis
Around 200,000 veterans suffer from Gulf War Illness (GWI). GWI is characterized by multiple deficits in cognitive, emotion, somatosensory and pain domains. In this study we studied 23 GWI patients and 30 age-matched controls with resting state fMRI in order to classify patients versus controls using functional connectivity among brain networks. Results show that different brain networks have discriminating power, signaling widespread impairments in functional connectivity of visual, semantic, multi-sensory, and sensory-motor processing networks in GWI consistent with multi-symptom nature of the illness.
INTRODUCTION
Gulf War Illness (GWI) is a chronic medical condition characterized by multiple symptoms which indicate brain function deficits in emotion, cognitive, pain and somatosensory domains1-3. It affects approximately 200,000 of the 1991 Gulf War veterans. Prior neuroimaging studies confirm presence of structural, functional and metabolic brain impairments in GWI4-6; however, GWI is still poorly understood. During the last two decades, functional neuroimaging technology, especially functional magnetic resonance imaging (fMRI), has improved tremendously, with recent attention towards resting-state functional connectivity (FC) analysis of the brain combined with independent component analysis (ICA)7-9. ICA can reveal which parts of the brain act as (statistically) independent functional networks7. FC analysis, based on ICA, can provide insight into overall functional connectivity between networks; differences in the FC of the brain networks under different brain conditions can be studied and used as features for classification9. In this study we used ICA-based FC as features to classify the GWI patients from normal control (NC) veterans.
METHODS
23 GWI veterans (mean age 49.4 yrs.) and 30 normal controls (NC) (mean age 49.8 yrs.) were scanned in a Siemens 3T Tim Trio MRI scanner using a 12-channel receiver head coil. Written informed consent was obtained from all participants in the protocol approved by the local Institutional Review Board. Whole-brain resting-state fMRI (rsfMRI) data were acquired with a 10-min whole-brain gradient echo EPI (TR/TE/FA = 2000/24ms/90°, resolution = 3mm×3mm×3.5mm). RsfMRI preprocessing steps included attenuation of signal related to subject-motion and physiological responses, using advanced ICA-based artifact reduction techniques, and spatial smoothing with FWHM = 6mm isotropic Gaussian kernel. Group spatial ICA10 were performed separately for each group, the number of independent components (ICs) were determined (21 ICs for NC and 23 ICs for patients) using the minimum description length criteria7. Subsequently, an overall combined group spatial ICA was done with the total number of ICs (44), which results in a higher dimensional estimation of the ICs11. After removal of 5 ICs which correspond to artifacts, the remaining 39 ICs were paired to obtain $$$\left(\begin{array}{c}39\\ 2\end{array}\right)=741$$$ FC values, which were used as initial features. The features were ranked and reduced to only 4 features (FC pairs) by using the Wrapper subset evaluator with "best-first" forward-search utility in Weka machine learning toolbox12. Classification was performed using the reduced number of features and different machine learning algorithms and cross-validation parameters using Weka.RESULTS
Combined group spatial ICA, when unrestricted, resulted in 22 ICs using the MDL criterion. Group spatial ICA with higher dimension of 44 ICs therefore corresponds to a 100% dimensionality increase when compared to the the unrestricted ICA. Five ICs were mostly artifactual and were removed from the classification analyses. After feature reduction to 4 FCs as described in the Methods section, using 10-fold cross-validation, a Naive Bayes Classifier algorithm classified 28/30 of NC and 19/23 of the GWI correctly, which corresponds to sensitivity of 82.6%, specificity of 93.3%, and an overall classification accuracy of 88.7%. Naive Bayes classification performed better than other algorithms in Weka. The 4 most discriminating FC pairs were the following:
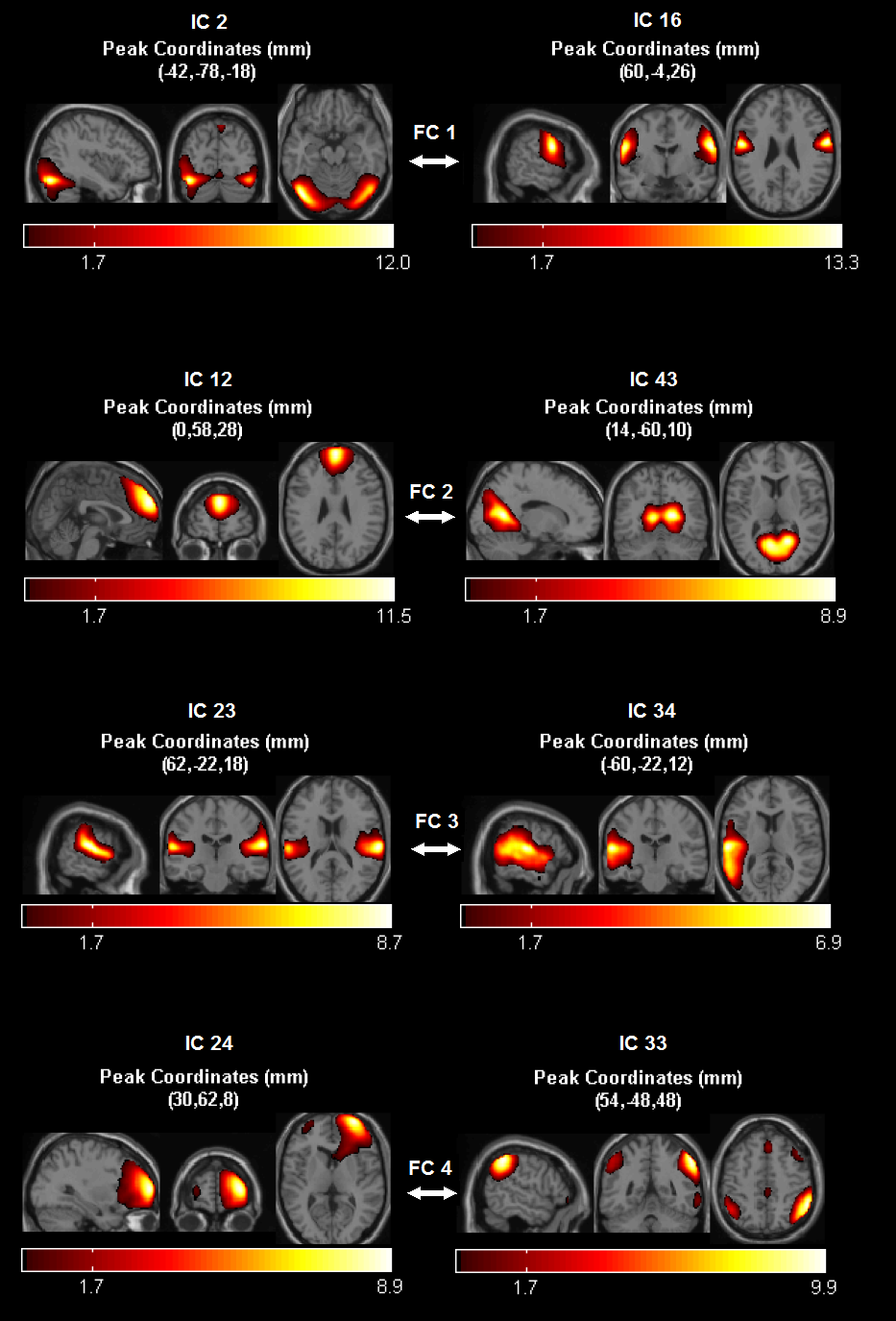
FC1: IC2 (higher visual content processing areas) & IC16 (motor cortex);
FC2: IC12 (superior frontal, anterior medial frontal) & IC43 (visual association cortex, retrosplenial cortex, posterior parahippocampal area; posterior cingulate);
FC3: IC23 (bilateral Sylvian fissure, superior temporal gyrus) & IC34 (left middle and superior temporal gyrus, mid and posterior);
FC4: IC24 (right lateral frontal cortex) & IC33 (right parietal, pre-sensory-motor, fronto-parietal, posterior mid cingulate cortex).
Mean FC values for the NC were higher than GWI for these FCs (p<0.05 for FC1 and FC4).
DISCUSSION AND CONCLUSION
Functional connectivity between multiple brain networks appeared as having good group discriminating power of 88.7%. FC1 is between higher visual processing areas and motor cortex; which is important for visuo-motor function, and multisensory processing. FC2 could be related to top-down influence on visual functions. FC3 could be related to auditory and language functions. FC4 could be related to fronto-parietal and task-positive networks. Overall, these regions were previously shown to be involved in either visual, auditory, sensory-motor input processing, or semantic processing. Consistent with these findings, GWI veterans were reported to exhibit deficits in word-finding13, in visual processing14, and in fine motor skills1. However, brain networks involved in successful classification need to be further interpreted and studied. Future work involves different feature/FC selection and classification algorithms to achieve a higher classification accuracy. Overall, the results are in line with other recent findings of widespread impairments in rsFC within brain function networks implicated by multiple symptoms in GWI patients1-6,13,14.
Acknowledgements
This work was supported by the Office of Assistant Secretary of Defense for Health Affairs, through the Gulf War Illness Research Program under Award No. W81XWH-16-1-0744 (PI: Gopinath). Opinions, interpretations, conclusions and recommendations are those of the author and are not necessarily endorsed by the Department of Defense.References
[1] Binns JH, et al., Report of Research Advisory Committee on Gulf War Veterans’ Illnesses, In: Affairs DoV, editor, Boston, MA, U.S. Government Printing Office, 2014.
[2] Haley RH, et al., JAMA, 277: 215-222, 1997.
[3] Toomey R, etal., J Int Neuropsychol Soc., 15:717-729, 2009.
[4] Moffet K, et al., Brain Cogn. 98:65-73, 2015.
[5] Gopinath K, et al.,Neurotoxicology, 33:261-71, 2012.
[6] Li X, et al., Radiology, 261:218-225, 2011.
[7] Calhoun VD, et al., HBM, 14:140–151 (2001).
[8] Jafri MJ, et al., Neuroimage, 39(4): 1666–1681 (2008).
[9] Sakoglu U, et al., MAGMA, 23(5-6): 351–366 (2010).
[10] http://mialab.mrn.org/software/gift
[11] Dipasquale O, et al. Front Hum Neurosci 9:43:1-7 (2015).
[12] https://www.cs.waikato.ac.nz/ml/weka
[13] Moffett K, et al. Brain Cogn 98:65-73 (2015).
[14] White RF, et al. Am J Ind Med 40:42-54 (2001).
Figures