5528
Feasibility Study of Arterial Spin Labeling on a Compact 3T Scanner with High-Performance Gradient System1Radiology, Mayo Clinic, Rochester, MN, United States, 2GE healthcare, Waukesha, WI, United States, 3GE Global Research, Niskayuna, NY, United States
Synopsis
Our study shows that pCASL based on a 3D segmented fast spin-echo spiral sequence can be performed on a compact 3T (C3T) scanner without the need of second RF transmitter. The high performance gradient system on the C3T can reach 80 mT/m magnitude and 700 T/m/s slew rate without peripheral nerve stimulation, which helps to shorten both the TE and spiral readout length. Both the perfusion-weighted images and the cerebral blood flow maps acquired on the C3T have higher spatial resolution and less off-resonant artifacts compares to those acquired on the conventional whole-body system enabled by the high performance gradients.
INTRODUCTION
There has been a rapid growing clinical interest of using arterial spin labeling (ASL) to characterize brain perfusion (1-4). By labeling the arterial blood spins prior to their inflow into the tissue of interest, ASL can provide quantitative perfusion information, obviating intravenous injection of contrast. Among various implementation strategies, the pseudo-continuous ASL (pCASL) combined with background suppression and segmented 3D readouts has gained popularity due to its high labeling efficiency and signal-to-noise ratio (SNR) (4).
A novel compact 3T scanner (C3T) was developed recently to meet the clinical demands for a lightweight, low-cost and high-performance MR system (5-7). The C3T was designed with a 37 cm bore and 26 cm diameter of spherical volume. It is equipped with a high-performance gradient system allowing for 80mT/m amplitude and 700T/m/s slew rate (SR) simultaneously (6). The built-in RF transmit/receive coil excites ±15cm from isocenter, which allows whole-head excitation and down to at least the C2-C3 junction of the cervical spine. Clinical pCASL protocols usually require positioning of a thin labeling plane at ~2 cm below the base of the cerebellum. As it is close to the inferior periphery of the RF excitation zone of the C3T, a study was performed to investigate if 3D pCASL can be performed on the C3T scanner without the need of a second RF transmitter.
A 3D multi-shot fast spin-echo (FSE) stack-of-spiral pCASL sequence was employed. The advantages of the high-performance gradient system are explored, as maximum gradient magnitude and slew rate influence the duration of the spiral readout and the minimum echo time.
METHODS
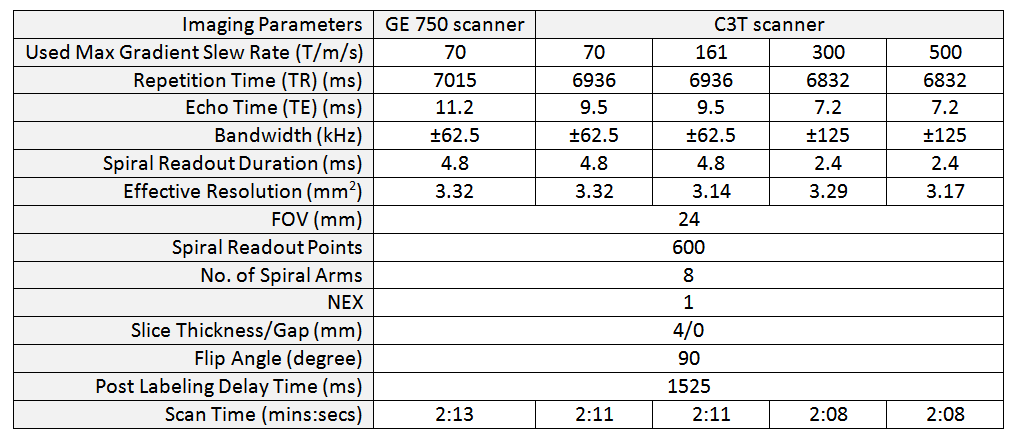
Under an IRB approved protocol, a healthy volunteer was scanned on a standard whole-body MR system (GE Discovery MR750, GE Healthcare, Waukesha, WI) and the C3T using an 8-channel receiver coil. On the whole-body system, the gradient SR for spiral readout was limited to 70 T/m/s by default to reduce peripheral nerve stimulation (PNS) risk (8). On the C3T, the PNS risk was much reduced due to its smaller imaging volume and therefore, a higher SR can be used for designing the spiral readout. To examine the effect of higher SR, a series of acquisitions were performed on the C3T with spiral readout gradient waveforms designed using different SR (161, 300, 500 T/m/s) and bandwidths ( ±62.5, ±125 kHz) (see table 1). The highest available gradient amplitude and SR on C3T was always used for other imaging gradients (e.g., crusher and phase encoding gradients). In all cases, an axial 3D pulsed-continuous ASL FSE spiral sequence was used. The imaging parameters are listed in table 1. Vendor-provided in-line reconstruction was used to reconstruct the raw images, the perfusion-weighted images and the cerebral blood flow (CBF) maps.RESULTS and DISCUSSION
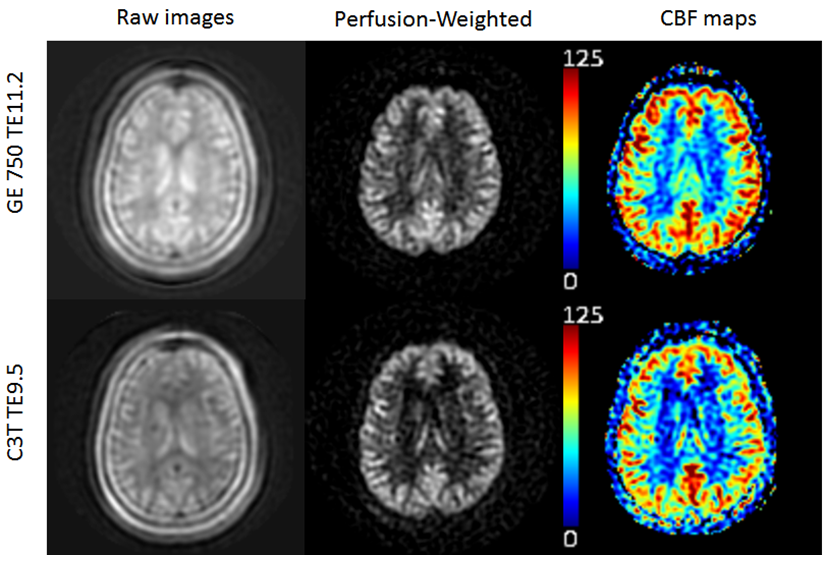
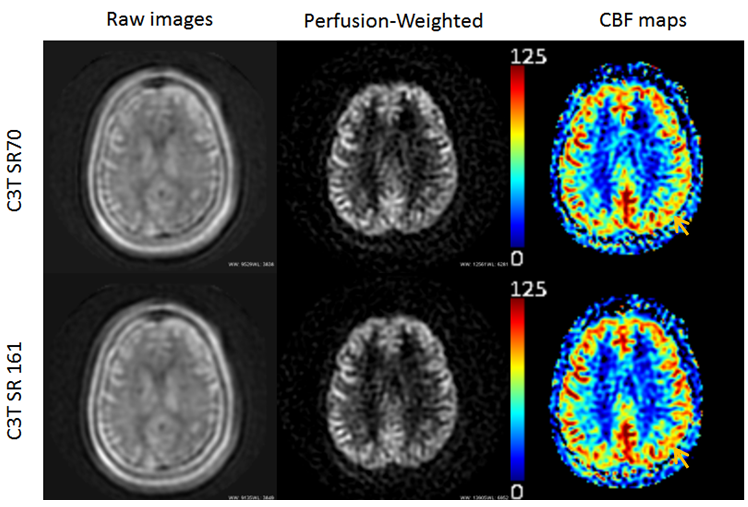
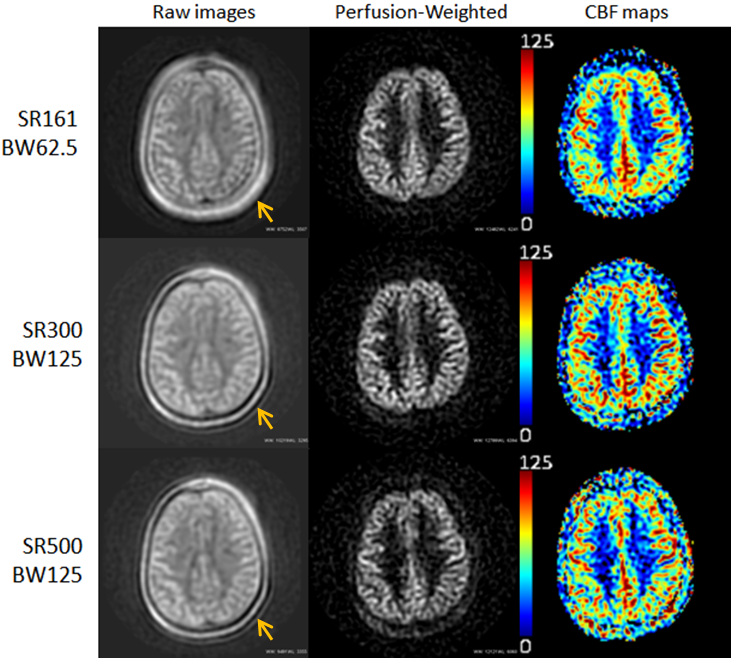
The raw images, perfusion-weighted images and the color-coded CBF maps for all cases are shown in figs. 1-3. All cases generated good quality brain perfusion images. Figure 1 compares the images acquired on the MR750 and the C3T systems using default gradient SR setup (70 T/m/s) at BW = ±62.5 kHz. A reduced TE (11.2 ms vs 9.5 ms) was achieved on the C3T due to higher gradient performance, which shortens the phase encoding and crusher gradients. Reduced T2-weighting and improved gray- to-white-matter ratio can be observed in the raw and perfusion-weighted images in Fig. 1. In Fig. 2, as the SR increased from 70 to 161 T/m/s, a slightly higher effective resolution was obtained (3.32 mm vs 3.17 mm). The CBF map using higher slew rate provides better visualization of the cortical region perfusion. Figure 3 demonstrates the trade-off between shorter readout using high SR/BW and SNR. Shorter readout (2.4 ms vs 4.8 ms) is especially effective in suppressing off-resonance effects caused by subcutaneous fat and visibly improves the delineation of the scalp and consequently enhances the perfusion signal. However, a higher readout BW and a reduced number of samples due to shorter readout time reduce the SNR, as shown in the bottom images. More signal averages could be used to boost the SNR. Also, higher SR is more prone to eddy current effects, so the fidelity of the spiral trajectory could potentially suffer. Based on the results of this comparison, the combination of 300 T/m/s SR and ±125 KHz BW (middle row) was deemed to be optimal, in consideration of both SNR and spatial blurring.CONCLUSION
Our study shows that pCASL can be performed on the C3T without the need of second transmitter. The high performance gradient system helps to shorten both the TE and spiral readout length which leads to higher resolution and less artifacts.Acknowledgements
The authors thanked Dan Rettmann from GE healthcare for the aid in providing pulse sequence implementation.
This work was supported by NIH grants U01 EB024450-01.
References
1. Williams DS, Detre JA, Leigh JS, Koretsky AP. Magnetic resonance imaging of perfusion using spin inversion of arterial water. Proc Natl Acad Sci U S A 1992;89:212–216.
2. Deibler AR, Pollock JM, Kraft RA, Tan H, Burdette JH, Maldjian JA. Arterial spin-labeling in routine clinical practice, part 1: technique and artifacts. AJNR Am J Neuroradiol 2008;29:1228–1234.
3. Pollock JM, Tan H, Kraft RA, Whitlow CT, Burdette JH, Maldjian JA. Arterial spin-labeled MR perfusion imaging: clinical applications. Magn Reson Imaging Clin N Am 2009;17:315–338.
4. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: a consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn. Reson. Med., 73: 102–116.
5. Foo T, Tan ET, Schenck J, Graziani D, Laskaris ET, Vermilyea M, Sabourin C, Shu Y, Huston J, Bernstein MA. Novel High Performance, Compact 3.0T MRI System for Imaging the Brain. Military Health System Research Symposium (MHSRS), Orlando, FLA August 2016.
6. Lee S-K, Mathieu J-B, Graziani D, et al. Peripheral nerve stimulation characteristics of an asymmetric head-only gradient coil compatible with a high-channel-count receiver array. Magn Reson Med 2016;76:1939–1950.
7. Weavers PT, Shu Y, Tao S, Huston J, Lee S-K, Graziani D, et al. Technical Note: Compact three-tesla magnetic resonance imager with high-performance gradients passes ACR image quality and acoustic noise tests. Med Phys 2016;43:1259–64.
8. King, K. F. and Schaefer, D. J. Spiral Scan Peripheral Nerve Stimulation. J. Magn. Reson. Imaging, 2000;12: 164–170.
Figures