5420
A simple semi-quantitative scale for brain MR imaging is associated with motor function, communication and cognition in dyskinetic cerebral palsy1Departament de Psicologia Clínica i Psicobiologia, Universitat de Barcelona, Barcelona, Spain, 2Institut de Neurociències. Universitat de Barcelona, Barcelona, Spain, 3Institut de Recerca Pediàtrica Hospital Sant Joan de Déu, Barcelona, Spain, 4IRCCS Stella Maris, Pisa, Italy, 5The University of Pisa, Pisa, Italy, 6Australian e-Health Research Centre. Commonwealth Scientific and Industrial Research Organisation, Brisbane, Australia, 7Departament de Psicologia Social i Psicologia Quantitativa, Universitat de Barcelona, Barcelona, Spain, 8Servei de Radiologia Pediàtrica. Hospital Universitari Vall d'Hebron, Barcelona, Spain, 9Grup de Recerca en Neurologia Pediàtrica. Vall d'Hebron Institut de Recerca. Universitat Autònoma de Barcelona., Barcelona, Spain, 10Queensland Cerebral Palsy and Rehabilitation Research Centre. Faculty of Medicine. The University of Queensland, Brisbane, Australia
Synopsis
Previous neuroimaging studies of DCP have been based on categorical descriptors or advanced neuroimaging protocols that cannot be easily utilised in a clinical context. To enable clinical translation, we characterized brain lesions, and their association with clinical outcomes in 39 participants with DCP, using a semi-quantitative scale for brain MRI that is clinically accessible due to its relative simplicity and reliance only on standard clinical images. Our results indicate that (A) ventral posterior lateral thalamus and frontal lobe are the most frequent locations of observable lesions in DCP and that (B) sqMRI can index motor, communication and cognitive functioning.
Introduction
Dyskinetic cerebral palsy (DCP) is the second largest cerebral palsy (CP) group (1). Although motor disturbances are the primary component of CP only a weak relationship has been found between motor severity and quality of life (2). Previous studies that utilised qualitative categorical descriptions of images have reported that the most frequent brain abnormalities observed in DCP are in the basal ganglia and thalamus, which in some cases are accompanied by periventricular leukomalacia, but some patients are without any apparent brain injury (3,4). Recent quantitative neuroimaging studies in DCP have demonstrated that white matter damage is common, and associated with lower motor and cognitive function. The translation of these findings to routine clinical practice is difficult because they rely heavily on specialised high quality images that are free of motion artefacts and require specialised processing. We aimed to (A) characterise a moderate-sized sample of participants with DCP using a semi-quantitative scale for brain structural MRI (sqMRI) (5), and (B) to examine the relationship between sqMRI scores and key clinical outcomes in CP: motor, communication and cognitive function.
Methods
Thirty-nine participants with DCP were assessed in terms of motor function, communication and a variety of cognitive domains. Whole-head MR imaging was performed for all participants in the form of fluid attenuated inversion recovery images (25 axial slices) and T2 turbo spin echo axial plane images. The sqMRI has been tested for reliability (5) and construct validity in unilateral CP (6) and can be scored despite certain movement artefacts that are highly likely to occur in DCP. Images were visually assessed and scored using the sqMRI by a MRI-trained neurologist. Ordinal, Poisson and negative binomial regression models were performed to identify which brain lesions accounted for specific clinical outcomes.
Results
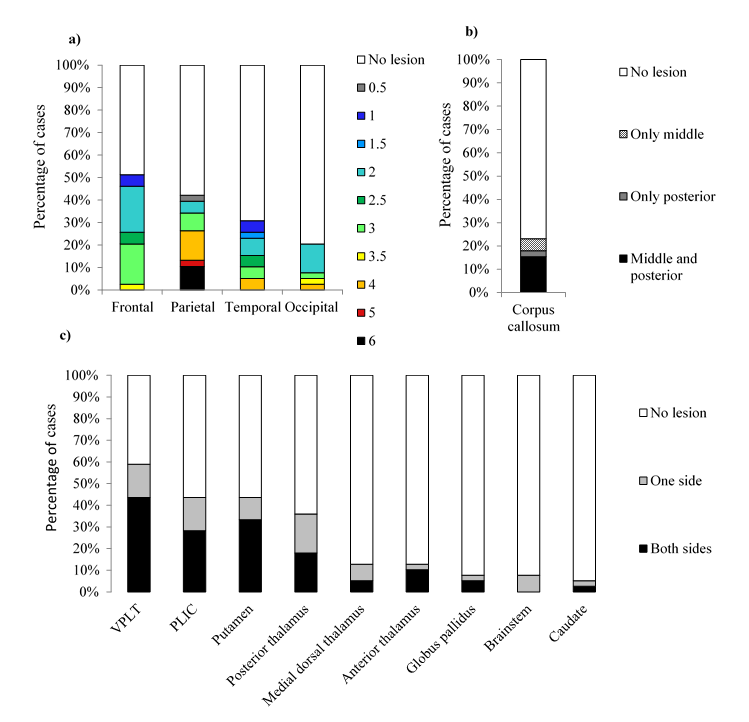
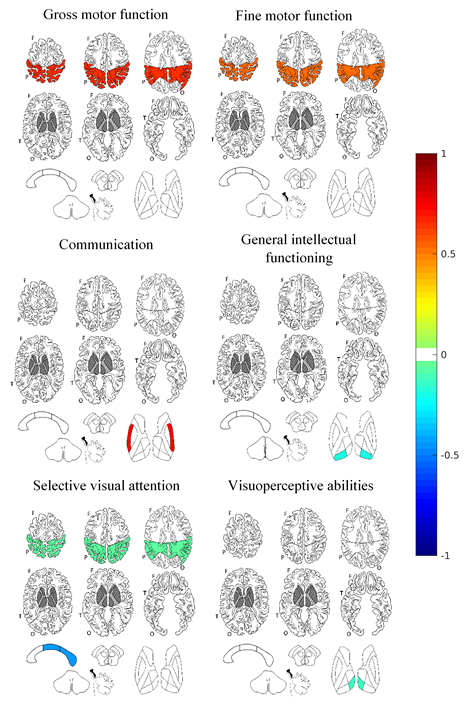
The two most frequent lesions were in the ventral posterior lateral thalamus and the frontal lobe (Figure 1). Global and parietal involvement was associated with gross (B=0.180, p<.001; B=0.658, p<.001) and fine (B=0.136, p=.003; B=0.540, p<.001) motor function (Figure 2). Putamen status was associated with communication functioning (B=0.747, p<.028). Intellectual functioning was associated with global sqMRI score and posterior thalamus involvement (B=-0.018, p<.001; B=-0.192, p<.001). Selective attention was associated with the global sqMRI score (B=-0.035, p<.001), the parietal score (B=-0.063, p=0.023), and corpus callosum score (B=-0.448, p<.001). Visuospatial and visuoperceptive abilities were associated with global sqMRI score (B=-0.078, p=.007) and medial dorsal thalamus status (B=-0.139, p<.012) respectively.
Discussion
This study identified the ventral posterior lateral thalamus, which is involved in sensory pathways (7), as the most common brain lesion in DCP. There are suggestions it critically supports an early visual pathway and plays a broad role in human cognition (8). In the present study, the posterior thalamic status was associated with intellectual functioning, as assessed by a visual reasoning task. In contrast, the medial dorsal thalamus and anterior thalamus were rarely injured, but sufficiently so that medial dorsal thalamic status was associated with visuoperceptive abilities. Parietal lobe lesions were more severe than frontal lobe lesions and were associated with poorer motor functioning. Lesions of the middle and posterior corpus callosum were associated with selective visual attention. Furthermore, damage occurring in the basal ganglia predominantly presented in the putamen which was associated with communication ability. These associations between lesions and clinical outcomes add credence to the potential clinical utilisation of the sqMRI. Given that lesions in CP are non-progressive, these results encourage replication of the current findings in a longitudinal study in which imaging is performed during infancy and clinical outcomes assessed during later childhood and adolescence. Conclusion Overall, our results indicate that (A) ventral posterior lateral thalamus and frontal lobe are the most frequent locations of observable lesions in DCP and that (B) motor, communication and cognitive functioning can be indexed by this simple clinically accessible lesion scoring system.
Acknowledgements
No acknowledgement found.References
1. Himmelmann K, McManus V, Hagberg G, et al. Dyskinetic cerebral palsy in Europe: trends in prevalence and severity. Arch Dis Child. 2009;94(12):921-926. 2. Shelly A, Davis E, Waters E, et al. The relationship between quality of life and functioning for children with cerebral palsy. Dev Med Child Neurol. 2008;50(3):199–203. 3. Krägeloh-Mann I, Cans C. Cerebral palsy update. Brain Dev. 2009;31(7):537–544. 4. Towsley K, Shevell MI, Dagenais L, Consortium R. Population-based study of neuroimaging findings in children with cerebral palsy. Eur J Paediatr Neurol. European Paediatric Neurology Society. 2011;15(1):29–35. 5. Fiori S, Cioni G, Klingels K, et al. Reliability of a novel, semi-quantitative scale for classification of structural brain magnetic resonance imaging in children with cerebral palsy. Dev Med Child Neurol. 2014;56(9):839–845. 6. Fiori S, Guzzetta A, Pannek K, et al. Validity of semi-quantitative scale for brain MRI in unilateral cerebral palsy due to periventricular white matter lesions: Relationship with hand sensorimotor function and structural connectivity. NeuroImage Clin. 2015;8:104–109. 7. Chien JH, Korzeniewska A, Colloca L, et al. Human Thalamic Somatosensory Nucleus (Ventral Caudal, Vc) as a Locus for Stimulation by INPUTS from Tactile, Noxious and Thermal Sensors on an Active Prosthesis. Sensors. 2017;17:1-22. 8. Bridge H, Leopold DA, Bourne JA. Adaptive Pulvinar Circuitry Supports Visual Cognition. Trends Cogn Sci. 2016;20(2):146–157.Figures