5399
Simultaneous Diffusion Tensor Imaging and T2 relaxometry in Lumbar Nerve Roots using Dual-Echo Single-Shot DW-EPI1Philips Japan, Tokyo, Japan, 2Radiology, Eastern Chiba Medical Center, Chiba, Japan, 3Division of Health Sciences, Graduate School of Medical Sciences, Kanazawa University, Ishikawa, Japan, 4Philips Healthcare Korea, Seoul, Korea, Democratic People's Republic of, 5General Medical Services, Chiba University Graduate School of Medicine, Chiba, Japan, 6Orthopaedic Surgery, Eastern Chiba Medical Center, Chiba, Japan, 7Philips Healthcare Asia Pacific, Tokyo, Japan
Synopsis
Diffusion tensor imaging (DTI) is promising for evaluation of lumbar nerve root compression in the extraforaminal area. A quantitative assessment using T2 relaxometry is also promising to evaluate nerve injury. Hence, nerve root quantification using both DTI and T2 relaxation properties may improve the diagnosis of nerve roots in patients with lower back pain, but it requires a long scan time. In this study, we developed a new sequence to simultaneously obtain both diffusion parameters and T2 value in one single scan (Diffusion-Relaxation Matrix: DRM). DRM simultaneously provides diffusion tensor imaging and T2 map without prolongation of acquisition time. This quantitative combination may be helpful to further assess the lumbar nerve root pathology.
PURPOSE
Lumbar nerve root entrapment caused by lumbar foraminal stenosis and disc herniation, commonly occur in the extraforaminal area1, can be a cause of low back pain; therefore, it is important to evaluate pathologic lesions in the extraforaminal area. Diffusion tensor imaging (DTI) based on a single-shot diffusion-weighted echo planar imaging (DW-EPI) is promising for evaluation of lumbar nerve root compression in the extraforaminal area. Several studies have shown that DTI and its tractography can visualize lumbar nerve disorders and quantitatively evaluate by using fractional anisotropy (FA)2-4. FA values is decreased at the nerve compression injuries due to nerve degeneration5.6. Besides, quantitative assessment using T2 relaxometry is also promising to evaluate nerve injury7-9. T2 values correlated with nerve injury and its functional recovery7. Hence, nerve root quantification using both DTI and T2 relaxation properties may improve the identification of the specific site of any degenerative and inflammatory changes along the nerve roots of patients with lower back pain10. However, in fact, a separate acquisition of DTI and T2 relaxometry requires long scan duration and it is hardly feasible in routine clinical examination.
In this study, we developed a new sequence to simultaneously obtain both diffusion related parameters and T2 value in one single scan (Diffusion-Relaxation Matrix: DRM). The purpose of this study was to evaluate the feasibility of DRM sequence.
METHODS
Theory and pulse sequence:
DRM is based on single-shot dual-echo DW-EPI sequence [Fig.1]. This sequence achieves dual echo-time (TE) by adding an extra refocusing pulse and EPI readout. Since motion-probing gradients (MPG) are applied around first refocusing pulse only, the effective diffusion time of both TEs are not changed. Accordingly, DRM reconstruction can simultaneously provide apparent diffusion coefficient (ADC) maps and FA maps of both short and long TEs (54ms and 120ms in this study), and T2 maps of both b=0s/mm2 and high b-value (b=800s/mm2 in this study) images in one single scan [Fig.2].
Experiments:
A total of five volunteers were examined with 1.5T whole-body clinical system (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects.
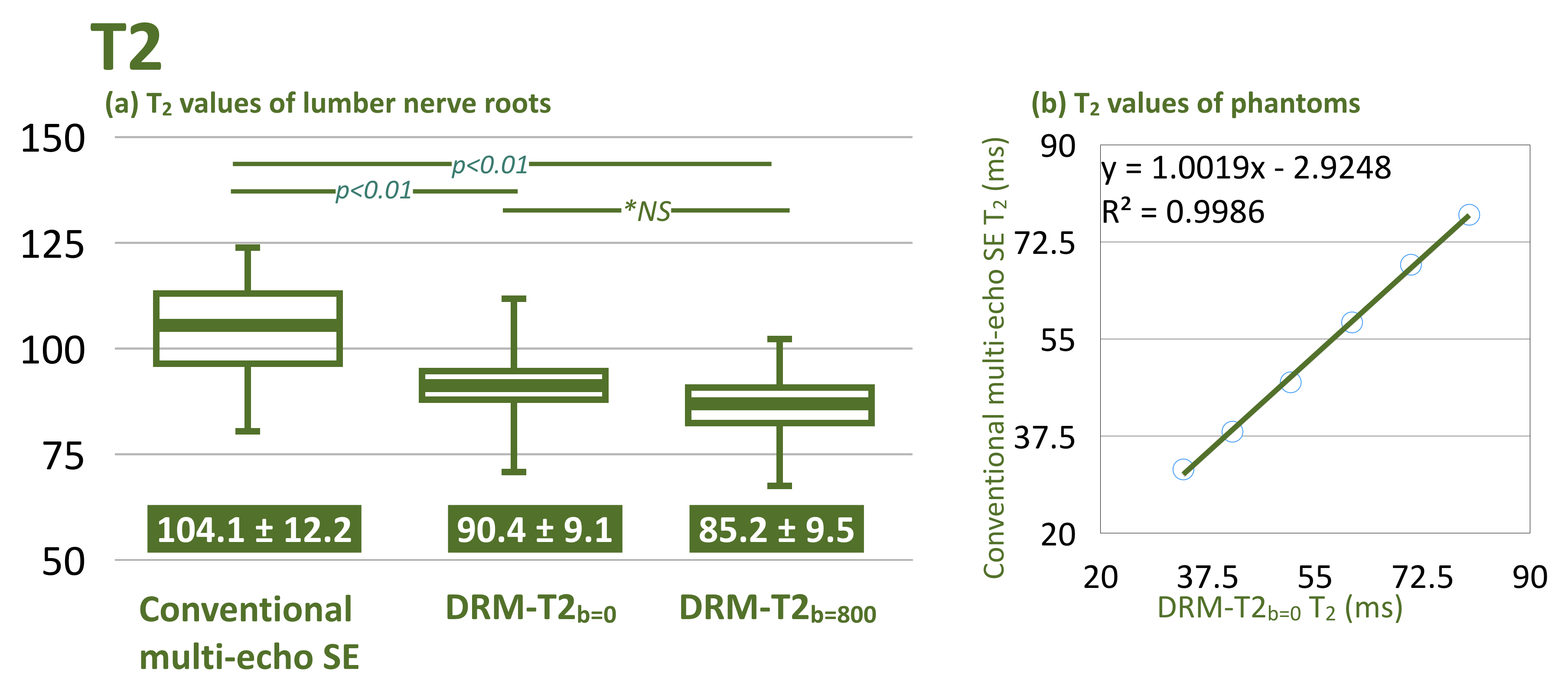
The T2 maps obtained by DRM sequence were assessed for accuracy by comparing with a conventional 2D multi-echo spin-echo (SE) T2 mapping sequence with use of dedicated phantom with various T2 values (filled with stepwise-diluted indigestible dextrin and soluble calcium) and human nerve roots. We measured the T2 value of the phantoms and nerve (average value of both the left and right dorsal root ganglions of L5 and S1). Spearman’s correlation coefficient in T2 values of phantoms were assessed. The T2 values were assessed by one-way repeated measures ANOVA and the post-hoc Tukey test. We also measured the ADC maps and FA maps with respective TEs and compared with the values reported in literature10-14.
Imaging parameters for DRM dual-echo DTI were: voxel size=3.33*2.21*3.50mm, FOV=320*253mm, 50 slices, b-value=0 and 800s/mm2, MPG=15 directions, TR=10900ms, TE=54 and 120ms, and total acquisition time=6m00s. Imaging parameters for multi-echo SE were: voxel size=1.5*1.8*3.5mm, FOV=320*253mm, 20 slices, TR=2600ms, TE=12ms*8, ETL=8, and scan duration=4min51s.
RESULTS and DISCUSSION
Fig.3(a) shows the comparison of T2 values among multi-echo SE and DRM-T2 with respective b-values. The T2 values of nerve in DRM-T2 with both b-values indicated slightly shorter time compared to those of conventional T2 mapping. The following points can be given as reasons. First, DRM calculated the T2 value by only two TEs. This may potentially cause unstable T2 assessments. Besides, partial volume effect, due to larger voxel size and image distortion of EPI, might also affect the measured T2 value. It is possible that T2 value changes due to the contamination from adjacent tissues. Nevertheless, the T2 values of dedicated phantoms measured in DRM-T2 well correlated with the one measured in multi-echo SE T2 mapping (R2=0.9986, P<0.01) [Fig.3(b)]. Thus, the T2 values measured in DRM-T2 may have same trends with one measured in conventional T2 mapping.
Fig.4 shows the FA and ADC values with respective TEs. Both the FA and ADC values with short TE indicated close to the values reported in literature10-14. These results suggest that the dual-echo acquisition does not adversely affect for assessment of these diffusion values. Furthermore, FA values were slightly decreased and ADC values are slightly increased by prolonging the TE [Fig.4]. Additionally, T2 values were slightly decreased due to the diffusion gradients [Fig.3(a)]. Although further clinical investigation is needed, these changes might be clinically useful in addition to FA, ADC and T2 values themselves.
CONCLUSION
DRM based on dual-echo DW-EPI sequence simultaneously provides diffusion tensor imaging and T2 map without prolongation of acquisition time. This quantitative combination may be helpful to further assess the lumbar nerve root pathology.Acknowledgements
No acknowledgement found.References
1. Heo DH, et al. Simple oblique lumbar magnetic resonance imaging technique and its diagnostic value for extraforaminal disc herniation. Spine 2009;34:2419–23.
2. Balbi V, et al. Tractography of lumbar nerve roots: initial results. Eur Radiol 2011;21:1153–9.
3. Eguchi Y, et al. Quantitative evaluation and visualization of lumbar foraminal nerve root entrapment by using diffusion tensor imaging: preliminary results. Am J Neuroradiol 2011;32:1824–9.
4. van der Jagt PK, et al. Architectural configuration and microstructural properties of the sacral plexus: a diffusion tensor MRI and fiber tractography study. Neuroimage. 2012;62:1792-9.
5. Khalil C, et al. Tractography of peripheral nerves and skeletal muscles. Eur J Radiol 2010;76:391–7.
6. Andreisek G, et al. Evaluation of diffusion tensor imaging and fiber tractography of the median nerve: preliminary results on intrasubject variability and precision of measurements. Am J Roentgenol 2010;194:W65–72.
7. Shen J, et al. MR neurography: T1 and T2 measurements in acute peripheral nerve traction injury in rabbits. Radiology. 2010;254:729–738.
8. Zhang X, et al. MR imaging and T2 measurements in peripheral nerve repair with activation of Toll-like receptor 4 of neurotmesis. Eur radiol. 2014;24:1145-1152.
9. Cha JG, et al. Median nerve T2 assessment in the wrist joints: preliminary study in patients with carpal tunnel syndrome and healthy volunteers. J Magn Reson Imaging. 2014;40:789-795.
10. Karampinos DC, et al. Diffusion tensor imaging and T2 relaxometry of bilateral lumbar nerve roots: feasibility of in-plane imaging. NMR Biomed. 2013;26:630-7.
11. Balbi V, et al. Tractography of lumbar nerve roots: initial results. Eur Radiol. 2011;21:1153-9.
12. Shi Y, et al. Diffusion tensor imaging with quantitative evaluation and fiber tractography of lumbar nerve roots in sciatica. Eur J Radiol. 2015;84:690-5.
13. Manoliu A, et al. Diffusion Tensor Imaging of Lumbar Nerve Roots: Comparison Between Fast Readout-Segmented and Selective-Excitation Acquisitions. Invest Radiol. 2016;51:499-504.
14. Eguchi Y, et al. Discrimination between Lumbar Intraspinal Stenosis and Foraminal Stenosis using Diffusion Tensor Imaging Parameters: Preliminary Results. Asian Spine J. 2016;10:327–334.
Figures
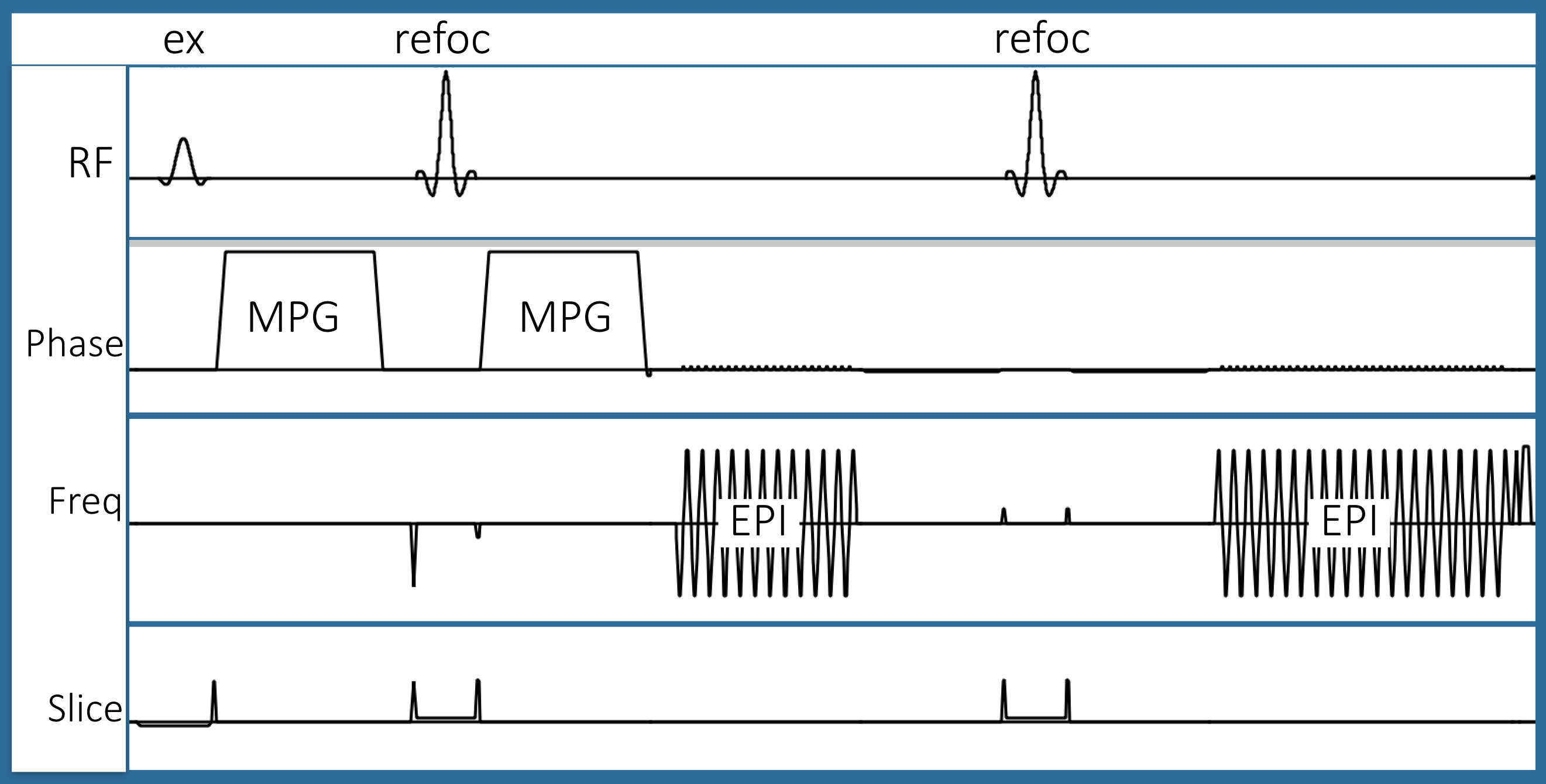
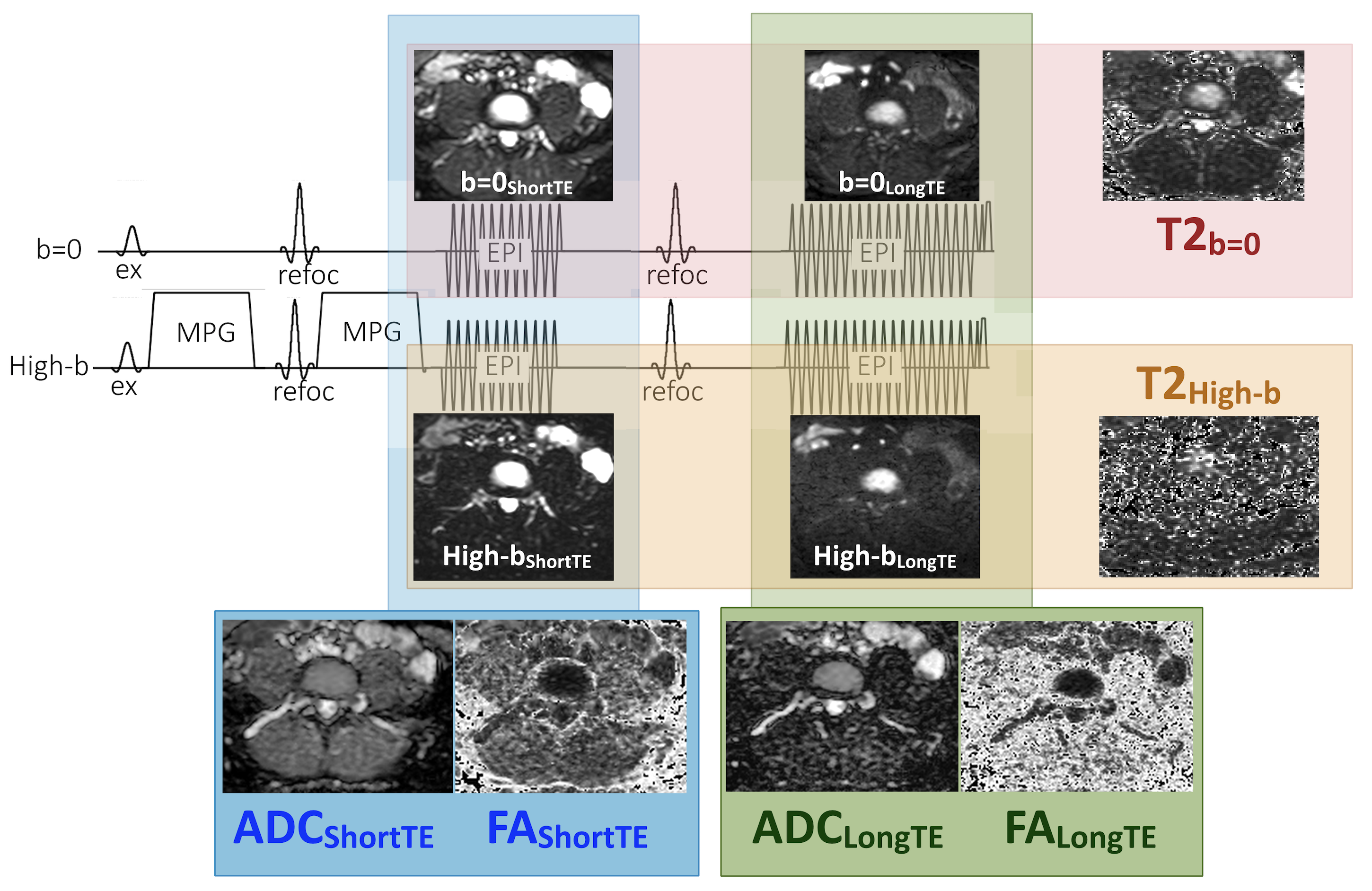
Fig.2. DRM reconstruction.
DRM simultaneously provides ADC maps and FA maps of both short and long TEs (54ms and 120ms in this study), and T2 maps of both b=0s/mm2 and high b-value (b=800s/mm2 in this study) images in one single scan.