5318
Functional Connectivity as a Potential Predictor of Treatment Response in Patients With Major Depressive Disorder1Huaxi Magnetic Resonance Research Centre (HMRRC) Department of Radiology West China Hospital, Chengdu, China
Synopsis
Resting-state functional connectivity(FC) analyses using a subcallosal cingulate cortex(SCC) seed was applied to major depressive disorder(MDD) patients to characterize a potential neuro-imaging biomarker that identifies the treatment outcome. MDD patients were divided into refractory and non-refractory group according to the treatment response. We found distinguished FC alterations between the three groups especially the lack of FC between SCC and Anterior Cingulate Cortex in the refractory MDD patients. In addition, the alterations in FC correlated with clinical symptoms in different ways in two MDD groups.
Purpose
Major depressive disorder is the second leading cause of disability worldwide, an estimated 15% of depressed individuals don’t respond to adequate treatment1. And some may evolved to treatment-refectory depression after several different therapies. Previous studies have demonstrated that Subcallosal cingulate cortex(SCC) may be a core component of depression pathophysiology and has consistently emerged as treatment target region2. In this study, we hypothesized that abnormal functional connectivity(FC) based on SCC as seed using resting-state fMRI would significantly different between refractory or non-refractory MDD patients and we would like to explore the exact region of difference between them. We will further correlate the FC changes with clinical symptom severity as measured by Hamilton Depression Rating Scale(HDRS) to explore the potential predictive value of this image marker.Materials and Methods
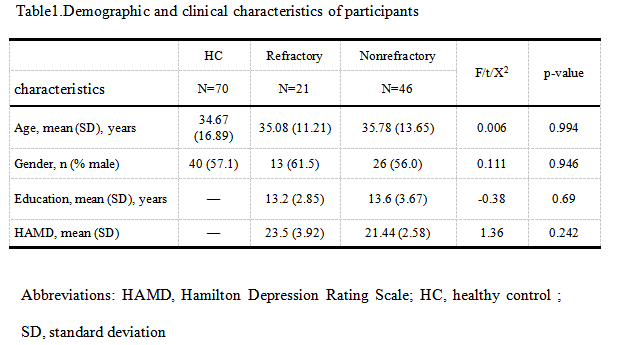
Participants: A total of 21 patients with refractory MDD,46 patients with non-refractory MDD, and 70 sex and age matched HC participated in the present study(Table 1). MDD patients were recruited from the Mental Health Center of West China Hospital and diagnoses were confirmed by using the Structured Clinical Interview for DSM-IV. Refractory depression is defined as a poor response after at least two trials with antidepressants from different classes and with adequate dosages. Details can be found in our previous publication3.
MRI Scanning: All MR data were collected with a 3T MR imaging system(GE). Resting-state functional MR were obtained using a gradient-echo sequence with below parameters:TR/TE=2000/30msec, FOV:240×240mm,flip angle=90°,slicethickness=5mm with no gap, 30 axial slices, 200 volumes in each run.
Data pre-processed and analysis: The functional MRI data were pre-processed using SPM8, and Data Processing Assistant for Resting-state fMRI (DPARSFA). We performed voxel-wise functional connectivity analysis using the REST toolbox . We chose SCC as individual seeds based on the coordinates suggested by Boadie W et al4( x=-6, y=24, z=-11, Radius=5mm). We used two-tailed one sample t-tests to compare each group’s SCC seed and whole-brain correlations, voxel based comparison of z-value maps among the three groups was performed using a design model of one-way analysis allowed by post hoc, two-sample t tests. Neuroimaging statistical analyses utilized a statistical height threshold of p< 0.05 and FWE correction (P < 0.05) at the cluster level. To examine the correlations between the connectivities and clinical variables, Pearson correlation were performed between these variables.
Results
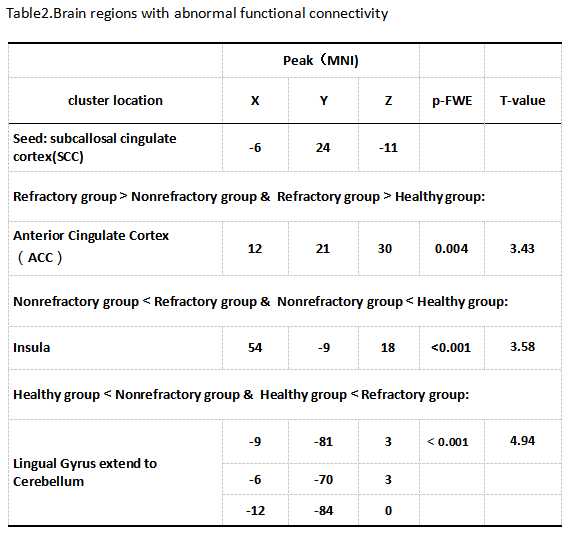
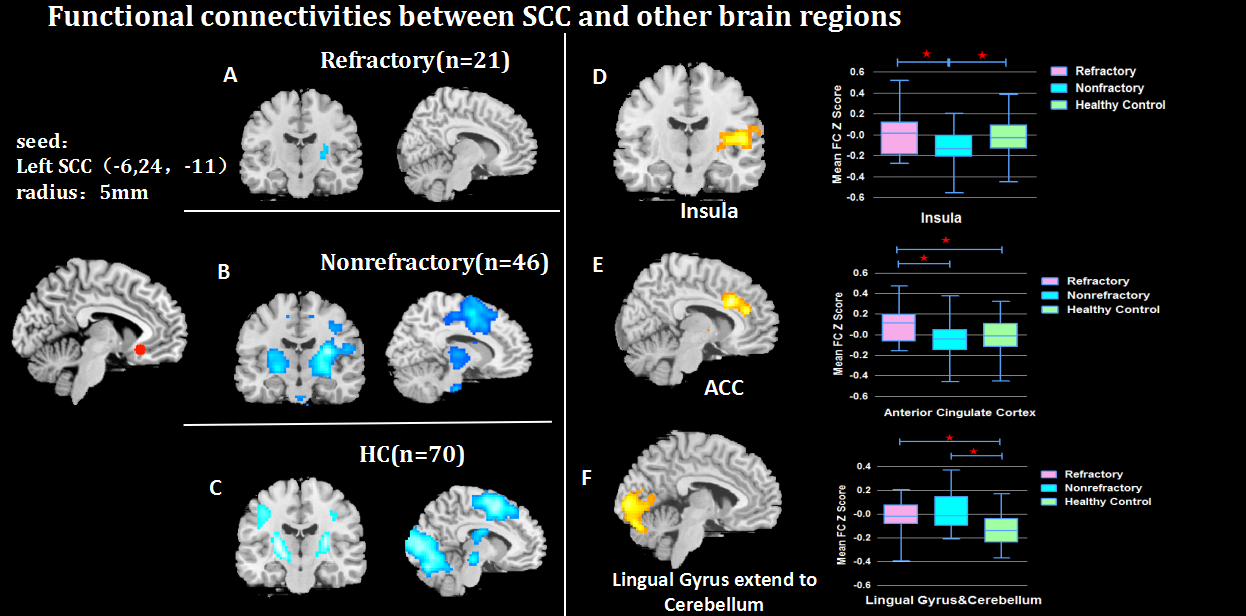
Iack of functional connectivity between SCC to ACC and insula in patients with refractory MDD: Relative to non-refractory MDD and healthy control group, refractory group showed no significant functional connectivity from SCC to Anterior Cingulate Cortex and insula(ACC).(Table 2 and Figure 1).
Negative functional connectivity between SCC and Lingual gyrus extend to cerebellum in healthy control: Relative to both patients groups ,healthy group showed significantly negative functional connectivity between SCC and bilateral Lingual gyrus extend to cerebellum.(Table 2 and Figure 1)
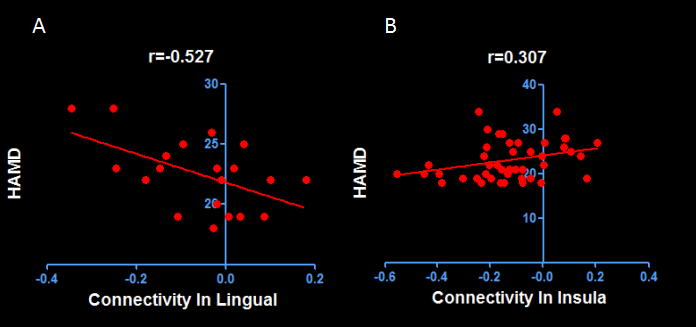
Correlations between between abnormal functional connectivity and clinical symptom: As shown in Figure 2, Negative correlation between FC in Lingual gyrus and the Hamilton Anxiety Rating Scale (HAMD) scores in patients with refractory MDD(r=-0.527,p=0.017). Positive correlation between FC in Insula and HAMD scores in non-refractory MDD patient group.(r=0.307,p=0.04) .
Discussion&Conclusion
This study demonstrated that the subcallosal cingulate cortex(SCC) plays a key role in major depression and have revealed aberrant patterns of resting-state functional connectivity in SCC. Our study yielded four main points. Firstly, the intra-group comparison have exhibited the abnormal functional connectivity among three groups. Secondly, the abnormal functional connectivity from SCC to ACC, Insula and Lingual gyrus would potentially differentiate treatment outcomes as refractory or nonrefractory. Thirdly, our correlational analysis suggested that abnormal connectivities between SCC and other regions might be associated with symptom severity. Finally, neuroimaging-based depression subtypes may be defined using SCC functional connectivity differentially identified the probability of treatment outcome. Further study is needed to investigate whether SCC functional connectivity would be explored as a biomarker of treatment prediction at the individual level.Acknowledgements
No acknowledgement found.References
1. The burden of depression. Nature 2014; 515:163.
2. Salerian AJ, Altar CA: The prefrontal cortex influence over subcortical and limbic regions governs antidepressant response by N=H/(M+R).Psychiatry Res 2012; 204:1–12
3. Lui S, Wu Q, Qiu L, Yang X, Kuang W, Chan R, Huang X, Kemp G, Mechelli A, Gong Q*. Resting-state functional connectivity in treatment-resistant depression. American Journal of Psychiatry. 2011, 168(6): 642-8
4.Boadie W. Dunlop, M.S., Justin K. Rajendra, et al.Functional Connectivity of the Subcallosal Cingulate Cortex And Differential Outcomes to Treatment With Cognitive-Behavioral Therapy or Antidepressant Medication for Major Depressive Disorder.Am J Psychiatry. 2017.
Figures