5309
Quantative Tractography Reveals Alteration in Corticospinal Tract Associated with Motor Abnormalies in Medication-Naive Attention-Deficit /Hyperactivity Disorder Children1Huaxi MR Research Center(HMRRC), Radiology Department, West China Hospital, Sichuan University, Chengdu, China, 2Department of Psychiatry, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou Medical University, Wenzhou, China
Synopsis
In the current study, we aim to quantify diffusion measures at multiple nodes along the trajectory of corticospinal tract in ADHD children. We found altered FA and RD in distinctive CST regions. Besides, significant correlations between neuropsychological measurements and abnormal white matter microstructure implicated critical role the disturbed CST played in the pathology of motor deficits in ADHD.
Background
Attention-deficit/hyperactivity disorder (ADHD), characterized by inattention and/or impulsivity-hyperactivity, is the most common neurodevelopmental disorder, diagnosed approximately in 5%–10% of children1. More than half of the children with ADHD have difficulties with gross and fine motor skills2. Alterations in white matter integrity were found in several parts of corticospinal tract(CST) suggesting involvement of the motor circuit in children with ADHD3,4. Hence, we employed a tract-oriented approach, namely automated fiber-tract quantification (AFQ)5 obtained from diffusion tensor image(DTI) to quantify diffusion measures at multiple nodes along the trajectory of CST in medication-naive ADHD children and try to find the association between fiber tract diffusion measurements and the motor cognitive functions.Methods
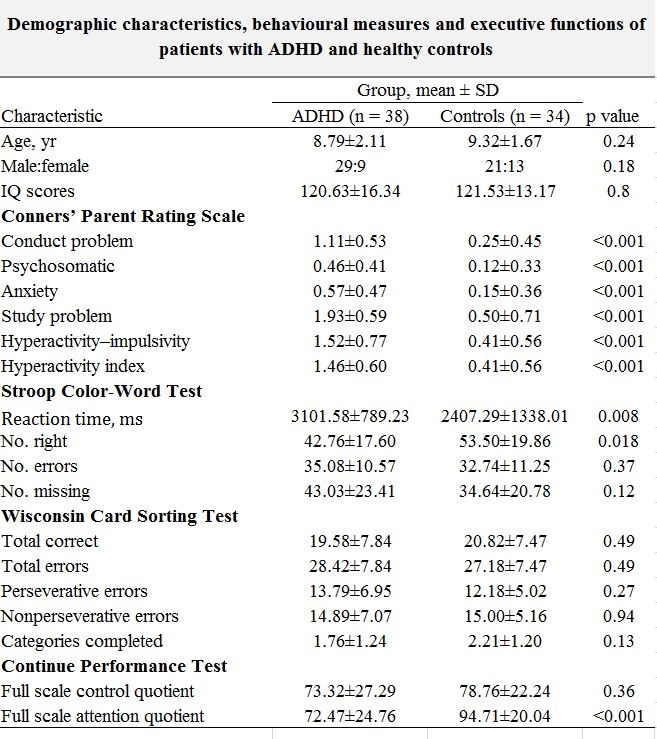
The study was approved by the local ethical committee and written informed consent was obtained from guardians of all subjects. Diagnosis of ADHD was determined by 2 experienced clinical psychiatrists using DSM-V. Subjects included thirty-eight drug-naïve ADHD children (mean ages 8.8±2.1 years, male: female=29:9) and thirty-four healthy controls (HC) matched for age, sex (mean ages 9.3±1.7 years, male: female=21:13). All participants had a full-scale IQ above 90 according to Weschler test, and there’s no difference in IQ scores between two groups. We used the Chinese version of revised Conners’ Parent Rating Scale (CPRS), Stroop Color-Word Test and Integrated Visual and Auditory Continue Performance Test (IVA- CPT) to assess problematic behavior, inhibitory control, and sustained attention and control, respectively.
All MRI scans were performed on GE signal HDx 3T MR scanner with an eight-channel phased-array head coil. The protocol included: (a) whole-brain T1-weighted scan MRI scanning (SPGR, TE/TR= 2.2/7.2 ms, flip angle =7°, 176 axial slices, slice thickness=1 mm); (b) diffusion-weighted imaging [EPI, TE/TR= 87.9/8875ms, 33axial-oblique slices, slice thickness= 4 mm, slice gap= 1mm, matrix size =130 × 128, FOV= 240 mm with 30 directions (b = 900 s/mm2) and 1 unweighted b0 scans (b=0s/mm2). Diffusion images processing was conducted by FSL to generate fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD) and radial diffusivity(RD), and a raw T2 signal with no diffusion weighting(S0). AFQ (github.com/jyeatman/AFQ) software package was then used for reconstructing the corticospinal tract (CST) and for evaluating diffusion metrics along the tract for both hemispheres. T-tests can be calculated point-wise along the tract for each diffusion metrics, and family wise error (FWE) correction (p<0.05) was applied to adjust for multiple comparisons. The association of each diffusion metrics (extracted from significant nodes between groups) with neuropsychological tests and behavioral assessment scales was evaluated using two-tailed Pearson correlation analysis.
Results
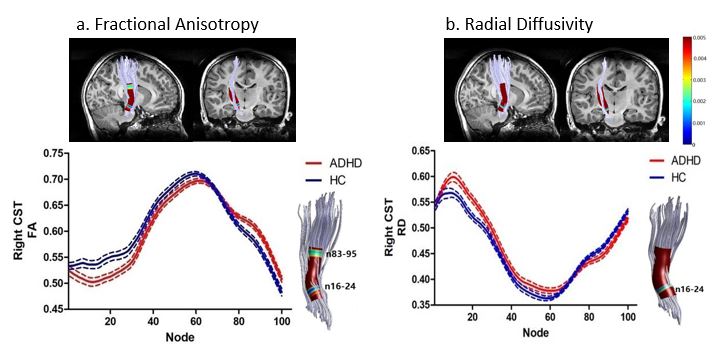
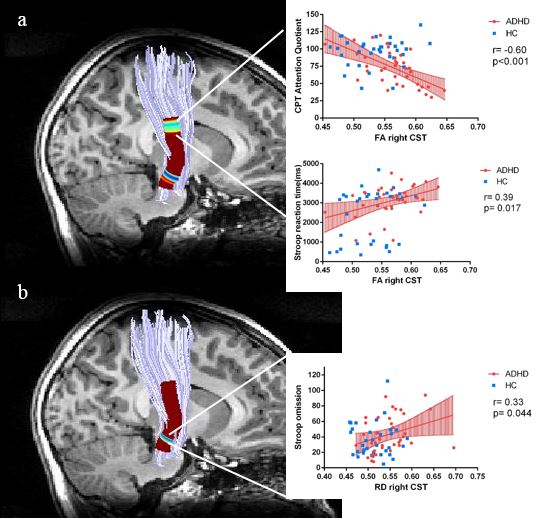
The ADHD group showed more severe behavioral problems and rated more poorly on neuropsychiatric test performance including more errors, longer reaction time and less attention focus compared to the ADHD group (Table1). ADHD children had significantly lower FA and higher RD on nodes 16–24(Figure 1a), while higher FA on nodes 83–95 for the right CST (Figure 1b). No group difference was observed for MD and AD values. Correlation analysis demonstrated a significant negative association between CPT attention quotient and FA values on nodes 85-95(r= -0.6, p<0.001), whereas positive correlation was observed between Stroop reaction time and FA on nodes 90-95 (r=0.39, p=0.017). On nodes 21-22 of the right CST, value of RD correlated positively with omission number in Stroop test (r=0.33, p=0.044) (Figure 2).Discussion
Rencent meta-analysise suggests that abnormalities in white matter might be an important factor in the pathophysiology of ADHD6. As far as we know, the present study is the first to examine microstructure integrity in CST in drug-naïve ADHD children. CST stretches between the primary motor cortex to the midbrain and is primarily involved in motor functions7. The two regions on the right CST which demonstrated altered FA in ADHD children were located at the posterior limb of internal capsule and the cerebral peduncle, suggesting involvement of the feedforward limb of the corticopontocerebellar circuit. It maybe the neural circuit involved in the pathology of motor deficits in ADHD.Conclusion
Overall, our study revealed the exact regions of CST contributed to the neuropathology of ADHD which may directly related to motor function.Acknowledgements
No acknowledgement found.References
1. American Psychiatric Association (2013): Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington, VA: American Psychiatric Publishing. 947 p.
2. Kaiser ML, Schoemaker MM, Albaret JM, et al. What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Res Dev Disabil. 2014;36C:338-357
3. Ashtari M, Kumra S, Bhaskar SL, et al. Attention-deficit/hyperactivity disorder: a preliminary diffusion tensor imaging study. Biol. Psychiatry. 2005;57(5):448-55.
4. Alena S, Igor N, Kyle R, et al. Unique White Matter Microstructural Patterns in ADHD Presentations—A Diffusion Tensor Imaging Study. Human Brain Mapping. 2016;37(9):3323-36.
5. Yeatman JD, Wandell BA, Mezer AA. Lifespan maturation and degeneration of human brain white matter. Nat Commun. 2014; 5:4932.
6. Aoki Y, Cortese S, Castellanos FX. Diffusion tensor imaging studies of attention-deficit/ hyperactivity disorder: meta-analyses and reflections on head motion. J Child Psychol Psychiatry. 2017 Jul 3.
7. King, JB, Yurgelun-Todd D, Stoeckel A, et al. Sex differences in white matter integrity in youths with attention-deficit/hyperactivity disorder: A pilot study. Frontiers in Neuroscience.2015; 9: 232
Figures