5270
Spinal cord cross section and DTI by vertebral level correlate superior and inferior to injuryDevon M Middleton1, Shiva Shahrampour2, Chris J Conklin1, Mahdi Alizadeh1, Scott H Faro3, Laura Krisa1, MJ Mulcahey1, and Feroze B Mohamed1
1Radiology, Thomas Jefferson University, Philadelphia, PA, United States, 2Bioengineering, Temple University, Philadelphia, PA, United States, 3Radiology, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Examination of diffusion and cord cross section by vertebral level in pediatric subjects has the potential to show useful information in injury diagnosis and prognosis. Correlations between DTI and cord cross section by vertebral level are shown superior and inferior to the injury site.
Introduction
Spinal cord injury (SCI) is a potentially debilitating condition, and is particularly problematic in the pediatric population where 50% of subjects with SCI have complete injuries with no motor or sensory function below the level of injury. Conventional MRI of the spinal cord can identify structural damage but does not reveal information relating to the injury process with respect to atrophy and microstructural changes. Diffusion tensor imaging (DTI) is increasingly used for examination of spinal cord injury and pathology, but it is often difficult to obtain DTI information at the site of injury due to the presence of metal hardware or the loss of cord tissue. Studies in the adult cervical cord have shown correlations with DTI and injury level in regions immediately adjacent injury [1] but no examination of the full pediatric cord by vertebral level has been performed. Examining DTI relationships with measurements of cord cross section may demonstrate that important information regarding the injury process is available superior and inferior to the injury site.Methods
Ten pediatric subjects with SCI were imaged using a Siemens Verio 3T MR scanner to acquire DTI data and high resolution anatomic scans covering the cervical and thoracic spinal cord (C1-T12). DTI was acquired using a tilted 2DRF inner-field-of-view EPI sequence [2] with parameters TE = 110 ms, TR = 7900 ms, diffusion weighted directions = 20, b = 800 s/mm2, voxel size = 0.8 x 0.8 x 6 mm3, axial slices = 40, averages = 3, b0 acquisitions = 6. Cardiac and respiratory gating were not used in order to keep scans as short as possible. For measurement of cord cross sectional area, a 3D TSE T2 weighted isotropic SPACE sequence was used with parameters TR = 1500 ms, TE = 122 ms, voxel size = 1 x 1 x 1 mm3. For both acquisitions, two volumes were imaged in order to cover the entire cervical and thoracic cord. DTI images were motion corrected and tensor estimation was performed using the RESTORE algorithm [3] to reduce the impact of outliers resulting from artifact. Cord cross section was measured using a semi-automated edge detection algorithm [4] for the entire spinal cord. DTI metrics were obtained from whole cord axial ROIs at each vertebral level. Fractional anisotropy (FA), axial diffusivity (AD), radial diffusivity (RD), and mean diffusivity (MD) were compared with cord cross section by vertebral level both above and below the injury site as determined by the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) examination.Results
Structural and DTI data were successfully acquired for subjects (Figure 1). Spearmann correlation tests were performed to examine significant relationships above and below the injury site between cord cross section and DTI metrics (Table 1). FA and cord cross section were strongly correlated both superior and inferior to the injury site. RD was moderately negatively correlated to superior to injury, and strongly negatively correlated inferior. MD was not significantly correlated to cross section superior to injury, but was moderately negatively correlated inferior to injury. AD was not significantly correlated in either case.Discussion
After injury, degenerative processes result in both atrophy observable at the macroscopic level and microstructural changes. The correlations of FA and RD with cord cross section are possible illustrations of the loss of white matter integrity during the atrophy process, where boundaries to isotropic diffusion degenerate. Further, the fact that these correlations exist superior and inferior to the injury site suggest that useful information regarding the injured spinal cord may be available even when the injury site cannot be imaged due to tissue loss or metal stabilization hardware. This is of particular interest in the case of longitudinal studies which may provide biomarkers during the injury recovery process.Conclusion
Correlations between cord cross section and DTI metrics by vertebral level suggest that imaging inferior and superior to focal spinal cord injury may yield useful information for diagnosis and prognosis.Acknowledgements
No acknowledgement found.References
1. Choe, et al. Subject-specific regional measures of water diffusion are associated with impairment in chronic spinal cord injury. Neuroradiology 2017.
2. Finsterbusch J. High-resolution diffusion tensor imaging with inner field-of- view EPI. JMRI 2009.
3. Chang L, et al. RESTORE: Robust estimation of tensors by outlier rejection. MRM 2005.
4. Liu W, et al. In vivo imaging of spinal cord atrophy in neuroinflammatory diseases. Ann Neurology 2014.
Figures
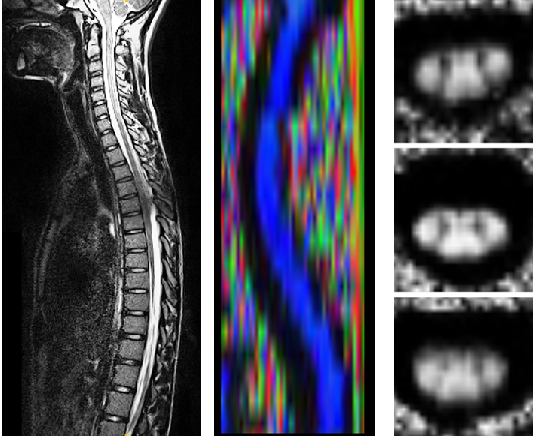
Figure 1 - Full T2 weighted 1mm isotropic cervical and thoracic spinal cord (left), representative sagittal color FA slab for cervical through mid thoracic cord (center), representative FA axial slices of spinal cord (right)

Table 1 - Spearmann correlation coefficients and associated p values between DTI measures and cord cross sectional area for vertebral levels superior and inferior to injury site.