5253
Brain Microstructure Characterization: Initial Experience and Optimization of protocols for the Siemens Terra 7T System1Chair of Cellular and Molecular Imaging, Comprehensive Heart Failure Center (CHFC), University Hospital, Wuerzburg, Germany
Synopsis
Recent technological advances have brought new ultrahigh-field MRI (UHF) systems to the market, which nourish the expectation of better image quality with vendor-supplied sequences than with older systems. This would be an important factor for a wider distribution of UHF system and, thus, for moving UHF technology forward from a research tool to a clinical application. Therefore, the aim of this study was to perform a pilot study to assess the new Siemens Magnetom Terra 7T system with regard to typical clinical applications of 7T MRI in the brain.
Introduction
Brain examinations have been in the center of performing elaborated studies at ultra-high field (UHF) for research purposes. Recent technological advances have brought new UHF systems to the market, which nourish the expectation of better image quality with vendor-supplied sequences. This would be an important factor for a wider distribution of UHF system and, thus, for moving UHF technology forward from a research tool to clinical applicability. Therefore, the aim of this study was to perform a pilot study to assess the new Siemens Magnetom Terra 7T system with regard to typical clinical applications of 7T MRI in the brain such as MPRAGE and SWI. Moreover, the strategy is to achieve a high resolution using the default sequences and to optimize them, based on the available literature and our own experience.Methods
Six microstructural pulse sequences and a default B1-map pulse sequence were acquired using a whole-body 7T scanner (Magnetom Terra, Siemens Medical Solutions, Erlangen, Germany).Thirteen healthy participants (20-41 years old) gave their written informed consent. Volunteers were scanned using a 1TX/32RX head Coil (Nova, Medical Solutions) and up to three sequences from those listed below. The study was conducted in accordance to the Declaration of Helsinki and obtained approval of the local ethics committee.
Magnetization prepared rapid acquisition gradient echo (MPRAGE)1 and MP2RAGE2 pulse sequences were selected based on two previous different studies. MPRAGE: TR=2500ms, TE=2.89ms, TI=1100ms, GRAPPA R=2, FA=7°, FOV=278mm, BW=350Hz/Px, 288 slices per slab, voxel size 0.8 mm3, TA=7.14 min. MP2RAGE: TR=5000ms, TE=3.21ms, TI1/TI2=800/2700ms, GRAPPA R=4, FA=5°/7°, FOV=270 mm, BW=240Hz/Px, 256 slices per slab, voxel size 0.5mm×0.5mm×0.7mm, TA=12.32min. DTI was adjusted to achieve 1mm isotropic resolution, a minimal TE and 30 diffusion directions after Skare3. DTI-RESOLVE: TR=5000 ms, TE1/TE2=64/100ms, GRAPPA R=3, 74 reference lines, FOV=220mm, BW=668Hz/Px, 35 slices, voxel size 1 mm3, TA=24.47min. The diffusion directions were acquired with a b-value of 1200 s/mm2. A deterministic fiber tracking algorithm4 with 60 degrees, 0.2 angular and anisotropy threshold respectively was applied using DSI Studio5. The step size was 0.5 mm. T2* and TSE sequences were modified after the literature sources. T2*/TSE: TR=1570/14300ms, TE=21/71ms, parallel MRI GRAPPA R=3, FA=52°/144°, FOV=240/23 mm, BW=50/257Hz/Px, 87/100 slices per slab, off/Turbo factor 7, voxel size 0.2mm×0.2mm×1.5mm/ 0.4mm×0.4mm×2mm, TA = 10.45/ 6.42min. SWI was adapted accordingly after Schmidt6 using a high-resolution. SWI: TR=27ms, TE=15ms, GRAPPA R=4, flip angle=15°, FOV=230mm, BW=140Hz/Px, 96 slices per slab, voxel size 0.2mm×0.2mm×1.5mm, TA=6.19min.
Results
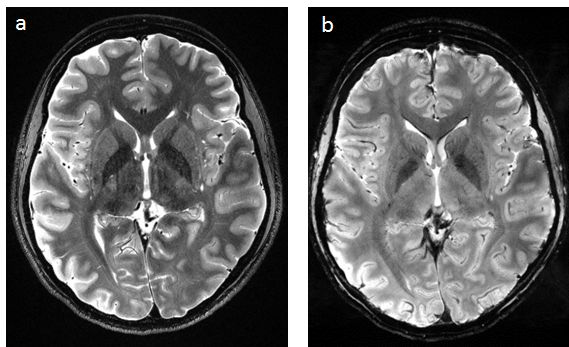
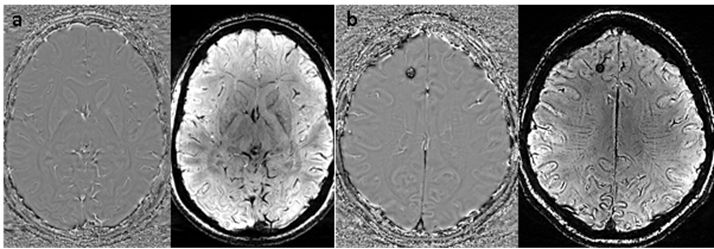
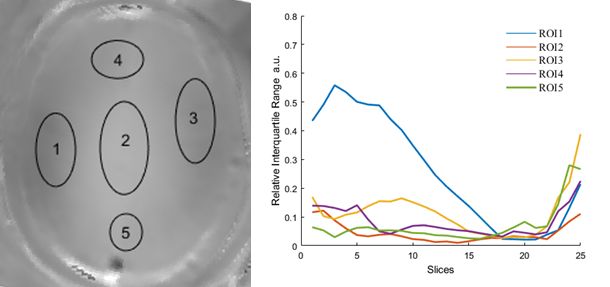
Figure 1 (a,b) shows typical MPRAGE/MP2RAGE images acquired with optimized standard protocol setting. As expected the MP2RAGE image quality is superior to MPRAGE. The fiber tracking reconstruction produced by RESOLVE DTI sequence is shown on Fig 2 overlapping ADC map. Both anatomical details with DW-contrast and fibers arrangements are well resolved. Figure 3 displays TSE-images providing both high resolution and T2-weighting contrast. The CSF, gray and white matter separation is very well distinguishable. Figure 4 shows T2* weighted images (phase and magnitude) providing high resolution reconstruction of susceptibility weighted (SW) image. Both contrast and spatial resolution provides high level of details in characteristic regions typically pronounced due to susceptibility effects. Figure 5 shows the B1-mapping results provided by standard “b1map” protocol based on saturation prepared turbo-FLASH. The 25 slices provides homogeneous map with a smooth distribution of flip angle.Discussion
As expected using two inversion times in MP2RAGE provides better image quality and better homogeneity of signal intensities compared to the conventional MPRAGE sequence. Therefore, subtraction image quality is well suitable for tissue segmentation according to clinical standard (b). RESOLVE led to longer scan times in comparison to a standard EPI sequence, but provided high quality diffusion weighted images. The angular resolution of fiber tracking benefited significantly from both 1mm3 isotropic voxel and SNR-gain achieved at 7T. Both T2 and T2* display a good contrast between regions of gray, white matter, and CSF. Moreover, the region that usually suffers from major signal losses due to high iron content, is perfectly contrasted. The B1 mapping measurement (Fig. 5) reveals that for most part of the brain, the homogeneous RF-excitation is provided with 10-15% of relative variation of B1. The lateral (ROI1 in Fig 5) part suffers from some inhomogeneity unclear origin, probably due to a TX or RX coil inhomogeneity. Nevertheless, further improvements employing B1-shimming provided by pTX capabilities of Terra is desirable.Conclusion
A clinical brain MRI examination protocol has been established at the new 7T system. Considering the field strength and use of single transmit technology rather than parallel transmit, image quality exceeded our initial expectation without major methodological improvements. Using 7T MRI to its full possibilities requires further research and is still work in progress.Acknowledgements
We acknowledge financial support of German Ministry of Education and Research (BMBF, grants: 01EO1004, 01E1O1504).References
1.Stefanescu M R, Dohnalek M, Maderwald S, et al., Structural and functional MRI abnormalities of cerebellar cortex and nuclei in SCA3, SCA6 and Friedreich’s ataxia. BRAIN 2015: 138; 1182–1197
2. Federau C, Gallichan D. Motion-Correction Enabled Ultra-High Resolution In-Vivo 7T-MRI of the Brain. 2016; PLoS ONE 11(5): e0154974. doi:10.1371/journal.pone.0154974
3. Skare S,Hedehus M, Moseley M E, et al. Condition Number as a Measure of Noise Performance of Diffusion Tensor Data Acquisition Schemes with MRI. Journal of Magnetic Resonance. 2000; 147(2): p. 340-352.
4. Schmidt M A, Engelhorn T, Marxreiter F, et al. Ultra high-field SWI of the substantia nigra at 7T: reliability and consistency of the swallow-tail sign. BMC Neurology 2017: 26;17(1)
5. Yeh, Fang-Cheng, et al. "Deterministic diffusion fiber tracking improved by quantitative anisotropy." (2013): e80713. PLoS ONE 8(11): e80713. doi: 10.1371
6. Yeh F-C. DSI-Studio. http://dsi-studio.labsolver.org. Accessed June 22, 2016.
Figures
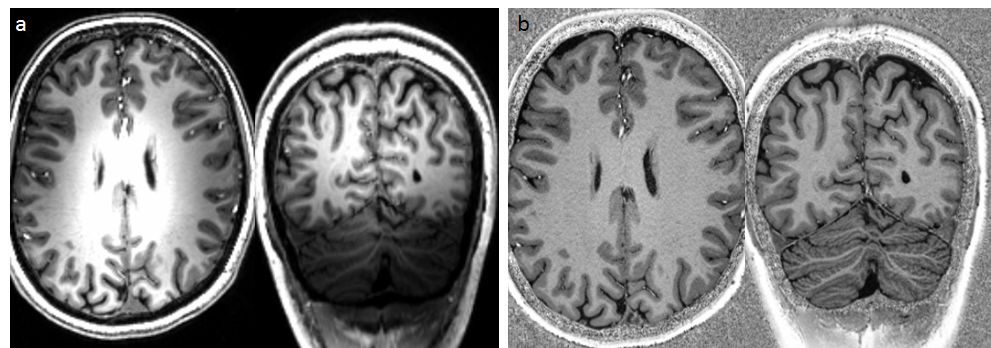
Fig 1. a) MPRAGE b) MP2RAGE
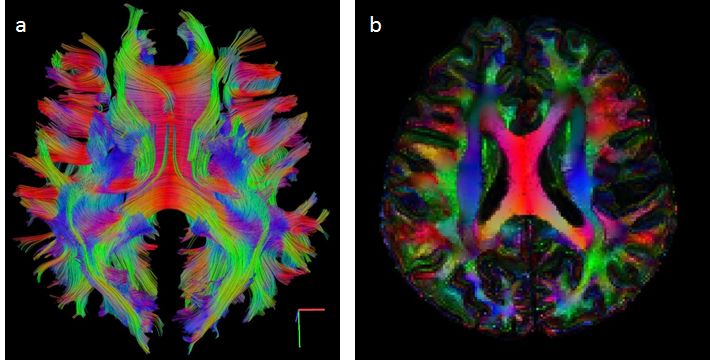
Fig 2. Fiber tractography using RGB color coding for the main eigenvector orientation b) Fractional anisotropy weighted map of the data in a.