5195
4D MSK MRI: Feasibility of Continuous and Pseudo Real-Time Imaging in the Shoulder and the Wrist1Radiology, UCSD, La Jolla, CA, United States, 2Toshiba Medical Systems, Otawara, Japan, 3VA San Diego Healthcare System, San Diego, CA, United States, 4Toshiba Medical Research Institute, Vernon Hills, IL, United States, 5Toshiba America Medical Systems, Tustin, CA, United States
Synopsis
For dynamic evaluation of musculoskeletal joints including the shoulder and the wrist, continuous and pseudo real-time techniques were developed in 4D (3D acquisition and time) using single shot FSE (SSFSE). Effective echo time (TEeff) of SSFSE was optimized for the contrast at each joint. Advantages of 4D over existing 2D techniques are volume acquisition with thinner slices, crucial in cases of target structures moving out of a single 2D imaging slice. Both continuous and pseudo real-time images permitted depiction of joint movements with good contrast; however, pseudo real-time gives slightly sharper images as compared to continuous real-time images.
Introduction:
There are several reports of 2D dynamic MR evaluation using FLASH, bSSFP, and single-shot FSE (SSFSE) in the musculoskeletal (MSK) system [1-5]. These are appealing for evaluating dynamic stabilization in joints, but have been limited to 2D applications with limited slice profile that cannot capture out-of-plane movement of imaging targets. In addition, although fast imaging with gradient echo (GRE) sequences like radial FLASH and bSSFP improves temporal resolution, susceptibility and off-resonance artifacts are inevitable. In addition, the contrast of bSSFP is fixed with intrinsic T2/T1 of complex MSK components and the freedom of contrast adjustment is challenging. These limitations are avoided with a spin-echo type SSFSE which is insensitive to off-resonance effects and has freedom of contrast optimization by varying effective TE (TEeff). In this project, our objective was to develop a 4D (3D volume + 1D time) technique with potential application in the shoulder's glenohumeral joint (GHJ) and the wrist.Methods:
MRI: 4D MR technique was developed for in vivo imaging at 3-T. A SSFSE sequence was developed for 1) pseudo real-time imaging by utilizing an intermittent SSFSE acquisition followed by a 2-sec pause during which the volunteer is instructed to move; and 2) continuous acquisition of real-time imaging using SSFSE. First, we qualitatively evaluated an effective TE (TEeff) between 10 ms and 60 ms to optimize the contrast in the GHJ and wrist, and decided on TEeff of 20 ms for both. In a healthy volunteer (male, 44 yrs old), we imaged GHJ in the axial plane during a very slow (continuous: a full cycle over 30 s) or an incremental (pseudo real-time: a full cycle over ~60 sec) medial rotation of right forearm with 3D SSFSE (TR=250 ms, TEeff=20 ms, echo train spacing (ETS)=5 ms, FA=90/160 deg, FOV=25 cm, matrix= 256(RO)x192(PE), slice=3 mm (15 slices), 0.4 (continuous) 0.21 (pseudo real-time) frames per second. Right wrist of the same volunteer was imaged in the coronal plane during ulnar-to-radial deviation movement with the same 3D SSFSE sequence except: TR=331 ms, TEeff=20 ms, FOV=22 cm, matrix=224x 224, slice=2 mm (10 slices). 3D Reconstruction: Images were imported into ImageJ, segmented for GHJ in shoulder images (no segmentation performed for the wrist), and 3D reconstructed (isosurface) to visualize joint movement.Results:
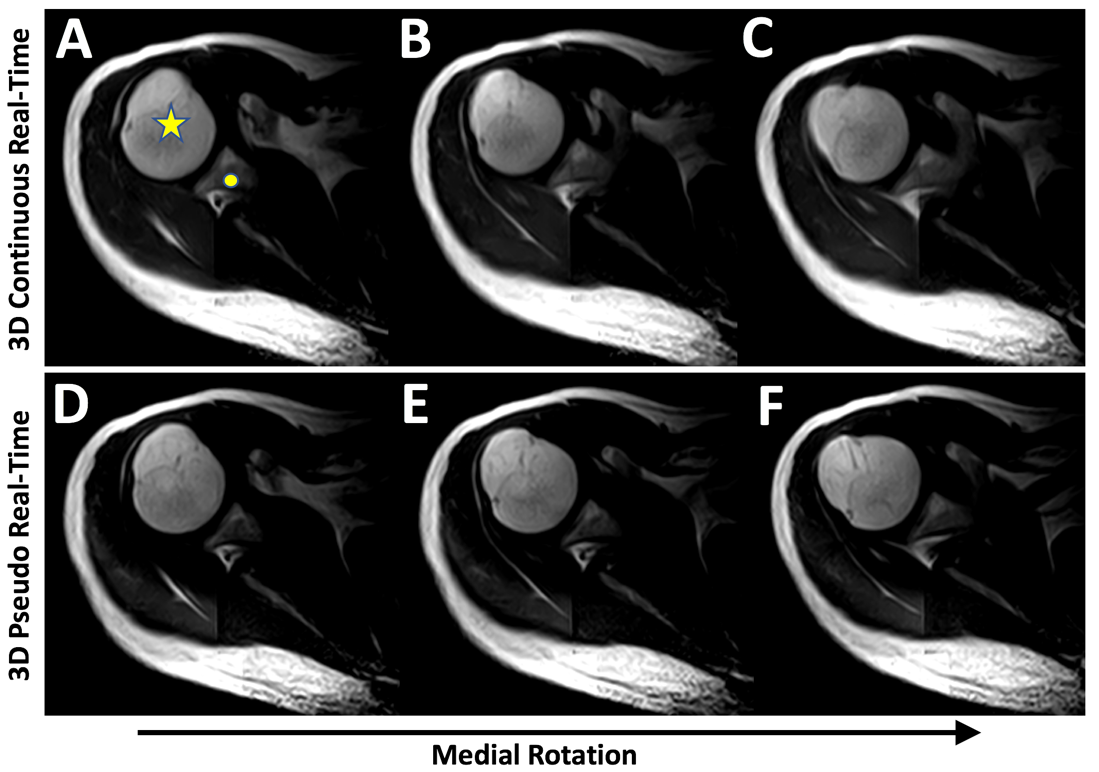
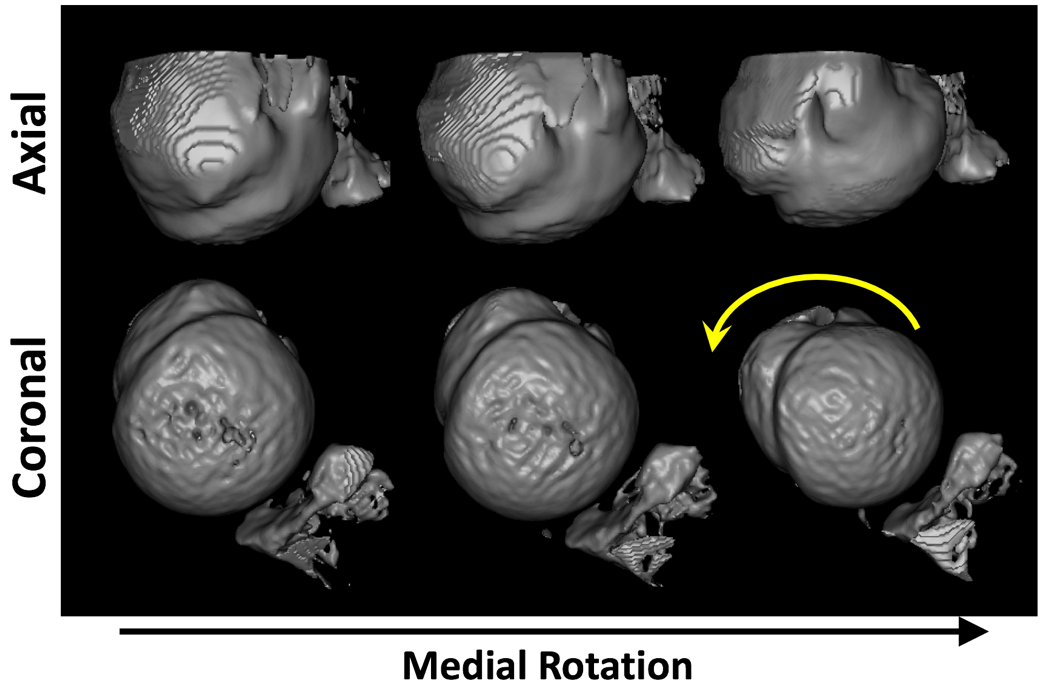
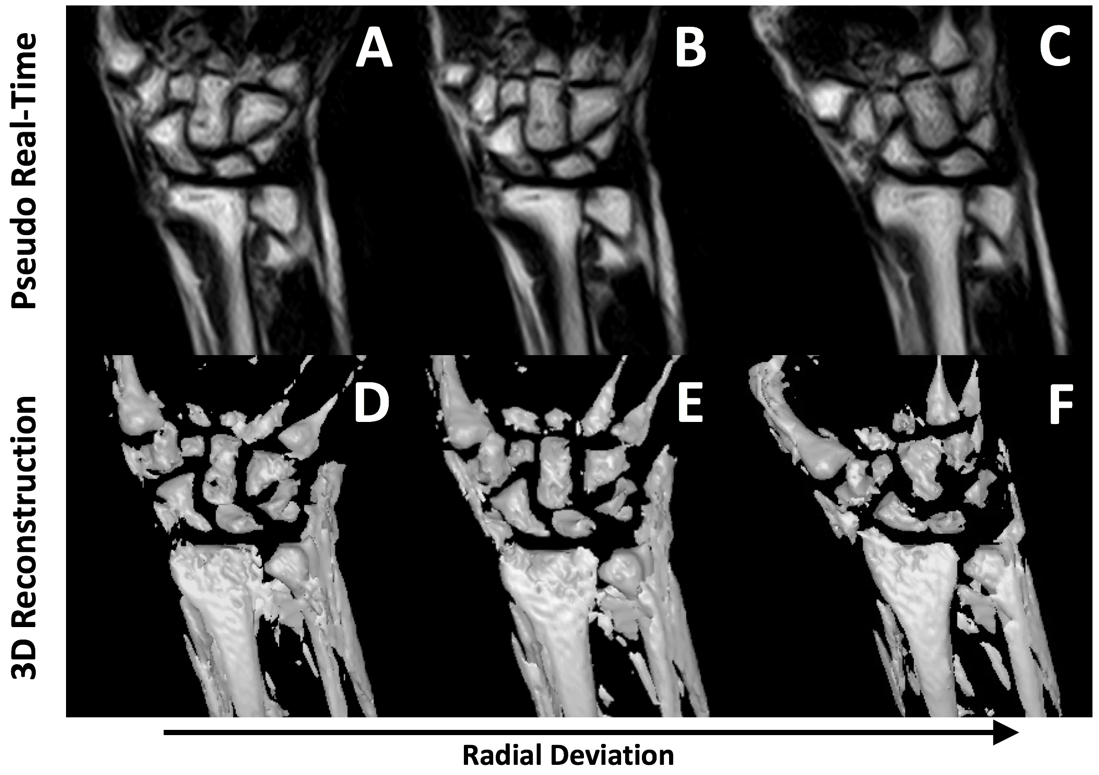
Both continuous (Figure 1ABC) and pseudo (Figure 1DEF) real-time 4D techniques yielded excellent contrast images of the GHJ and the wrist. Signal-to-noise ratio (SNR) was adequate; for example, in the GHJ, average SNR of the humeral head and surrounding muscle was 19.8 and 9.0, respectively. There was a moderate variation in SNR through the slice, evident by standard deviation in SNR of 7.4 and 3.7, respectively, for humeral head and muscle. Joint position and quality between the continuous and pseudo real-time images were similar, however, a slight blurring could be seen around the boundary of the humeral head in the continuous images (Figure 1BC). In the GHJ, changing orientation of humeral head (Figure 1A, star) and glenoid (Figure 1A, circle) during the forearm rotational motion is clearly seen. There was out-of-slice movement evident near the glenoid. Using 3D reconstruction (Figure 2), the entirety of the GHJ movement can be appreciated, and viewed from different perspectives. Similarly, in the wrist, ulnar-radial deviation movement can be seen with excellent contrast between carpal bones (Figure 3ABC), which can be volume-rendered (Figure 3DEF).Discussion:
This study demonstrates feasibility of 4D dynamic MR techniques for evaluation of MSK structures, in continuous and pseudo real-time fashion. 4D, compared to existing 2D dynamic techniques, has added advantages in cases where complex, out-of-slice motions are involved, such as biceps subluxation/dislocation in the GHJ or intrinsic ligament injury in the wrist. The technique also affords thin slices or isotropic imaging, albeit at a slower frame rate. In addition, 4D pseudo real-time technique with intermittent 3D SSFSE is feasible as a dynamic technique that may yield high resolution sharper images. There are situations where continuous technique is preferred, in joints such as the temporomandibular joint, where a pseudo dynamic motion has been shown to differ from continuous motion [6]. Our techniques are versatile and can adapt to different circumstances while maintaining similar image quality and contrast.Conclusion:
4D MR techniques enable dynamic imaging of MSK joints, providing new ways to evaluate these structures which were previously challenging with static or single-slice dynamic imaging.Acknowledgements
This work was supported, in part, by a grant from the Toshiba Medical Systems (16-01762).References
1] Boutin RD, Buonocore MH, et al. Plos One 2013; 8(12) e84004.
2] Shimazaki Y, et al. Magn Reson Med Sci 2007;6(1):15-20.
3] Sun Q, et al. Magnetic Resonance Imaging 2015;33:270-275.
4] Zhang S, et al. The open Medical Imaging Journal 2011;5:1-7.
5] Yen P, et al. AJNR Am J Neuroradiol 2013;34:E24–E26.
6] Seemann R, et al. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(3):371-8.
Figures