5188
Application of Intravoxel incoherent motion diffusion imaging in evaluation of tendon perfusionMichael Liu1, Patrick Quarterman1, Sachin Jambawalikar1, and Tony Wong1
1Columbia University, New York, NY, United States
Synopsis
Altered perfusion may be a marker of tendon damage. Measurable perfusion characteristics using non contrast techniques such as Intravoxel Incoherent Motion Diffusion Weighted imaging may be a useful technique for assessing perfusion characteristics of tendon.
Abstract
Intravoxel incoherent motion (IVIM) imaging has been proposed as a useful technique for assessing the perfusion and diffusion of muscles. Changes in IVIM parameters (f, D*, and D) are detectable in muscle following exercise. The aim of this work is to determine the selectivity and temporal evolution of f, D*, and D in the muscle-tendon unit following exercise.Background
Altered perfusion may be a marker of muscle and tendon damage. Therefore, measurement of perfusion may provide useful information in treatment or diagnosis of various muscle and tendon disease states2, 6. Intravoxel incoherent motion (IVIM) imaging has been proposed as a useful technique for assessing the perfusion and diffusion of muscles and tendons with detectable changes occurring in f, D*, and D parameters 3,6,7. The aim of this work is to determine the selectivity and temporal evolution of IVIM parameters in the forearm tendino-musculature following exercise.Methods
Eight volunteers (2 women and 6 men) ranging from the ages of 28 years to 51 years were scanned on a GE Healthcare 3.0T 70cm bore scanner (MR750W) using a 16 channel Small Flexible extremity phased array coil. The subjects were scanned in a lateral decubitus arm down position. Images were acquired in the axial plane perpendicular to the long axis of the forearm. An Anatomical T1 weighted fast spin echo (FSE) sequence was acquired with the following parameters: field of view 16cm x 16cm, Matrix 512 x 256, 26 slices, slice thickness 4mm and 0 gap, TR/TE:614ms/14.5ms, echo train length 4, receiver bandwidth 50kHz, parallel imaging (ARC) acceleration factor 1.5. Total scan time was 1 minutes 59 seconds. IVIM EPI sequence The standard product spin-echo single shot echo planar imaging (EPI) diffusion weighted (DW) was performed with the following parameters: field of view 16cm x 16cm, Matrix 80 x 80, 26 slices, slice thickness 4mm and 0 gap, TR/TE:3500ms/75.3ms, receiver bandwidth 166.7kHz, parallel imaging (ASSET) acceleration factor 2. EPI was acquired in 3 orthogonal directions at multiple b-values (0, 10, 20, 40, 80, 110, 140, 170, 200, 300, 400, 500, 600, 700, 800, 900 s/mm2), averaged 2 times for b-values (0 – 600) and 3 times for b-values (700 – 900). Total acquisition time was 5 minutes and 43 seconds. This series was conducted once prior to exercise and three times (0 minute, 10 minutes and 20 minutes) post exercise Exercise The volunteers were taken out of the scanner after the initial scans of T1 FSE and EPI-DW then seated with forearm in the prone position to perform a wrist flex maneuver for 2 minutes with a 5-pound dumbbell. Immediately after exercise, the volunteers were returned to the scanner in the same scanning position to complete the remaining EPI-DW scans. Image Processing All EPI DW images were deformably registered to the pre exercise b0 image using Advanced Normalization Toolkit1.. Mutual information was used as the similarity metric for registration and b-splines were used for interpolation. ROI’s were drawn on a single slice around the extensor carpi radialis brevis, extensor digitorum, extensor carpi ulnaris, and the common extensor tendon using MITK diffusion toolkit4. The IVIM model was fitted to each ROI with the same software. D and f parameters were initially fitted to the signal intensities of scans with b values higher than 170. These parameters were then used to fit D*.Results
Diffusion coefficient, pseudo-diffusion coefficient and perfusion fraction parameters derived from the extensor muscles and tendons are tabulated in Table 1. Student t-tests demonstrate that the changes in perfusion parameters in tendon between time points are not statistically significant. Student t-tests amongst parameters derived from extensor muscles shows D* parameters derived from extensor muscles as well as perfusion fraction derived from extensor carpi ulnaris are not statistically significant. Average values of individual muscle groups shows an increase in perfusion fraction from pre exercise to post exercise values and a decline of parameters from post exercise to 10 minutes and 20 minutes post exercise. Tendon perfusion parameters show that there is a trend toward elevated perfusion parameters following exercise.Conclusion
These results show the possibility of detecting perfusion changes in tendon with IVIM DW imaging. Though the changes detected in this experiment are not statistically significant, the trends corroborate physiological changes that would take place. The results also indicate that perfusion changes in tendon may evolve temporally differently than perfusion changes in muscle. As a whole we see that perfusion changes due to exercise are reflected in IVIM derived perfusion parameters corroborating results from previous papers indicating IVIM was a viable for detecting perfusion changes in muscle5.Acknowledgements
No acknowledgement found.References
1. Avants BB, Epstein CL, Grossman M, Gee JC. Symmetric diffeomorphic image registration with cross-correlation: evaluating automated labeling of elderly and neurodegenerative brain. Med Image Anal. 2008 Feb;12(1):26–41. 2. Challa ST, Hargens AR, Uzosike A, Macias BR: Muscle Microvascular Blood Flow, Oxygenation, pH, and Perfusion Pressure Decrease in Simulated Acute Compartment Syndrome. J Bone Joint Surg Am 2017; 99:1453–1459. 3. Filli L, Boss A, Wurnig MC, Kenkel D, Andreisek G, Guggenberger R: Dynamic intravoxel incoherent motion imaging of skeletal muscle at rest and after exercise. NMR Biomed 2015; 28:240–246. 4 Fritzsche, Klaus H., Peter F. Neher, Ignaz Reicht, Thomas van Bruggen, Caspar Goch, Marco Reisert, Marco Nolden, et al. “MITK Diffusion Imaging.” Methods of Information in Medicine 51, no. 5 (2012): 441. 5 Liu C, Liang C, Liu Z, Zhang S, Huang B. Intravoxel incoherent motion (IVIM) in evaluation of breast lesions: Comparison with conventional DWI. European Journal of Radiology [Internet]. 2013 Dec 1 [cited 2017 Nov 9];82(12):e782–9 6. Qi J, Olsen NJ, Price RR, Winston JA, Park JH: Diffusion-weighted imaging of inflammatory myopathies: polymyositis and dermatomyositis. J Magn Reson Imaging JMRI 2008; 27:212–217. 7. Nguyen A, Ledoux J-B, Omoumi P, Becce F, Forget J, Federau C: Selective microvascular muscle perfusion imaging in the shoulder with intravoxel incoherent motion (IVIM). Magn Reson Imaging 2017; 35:91–97.Figures
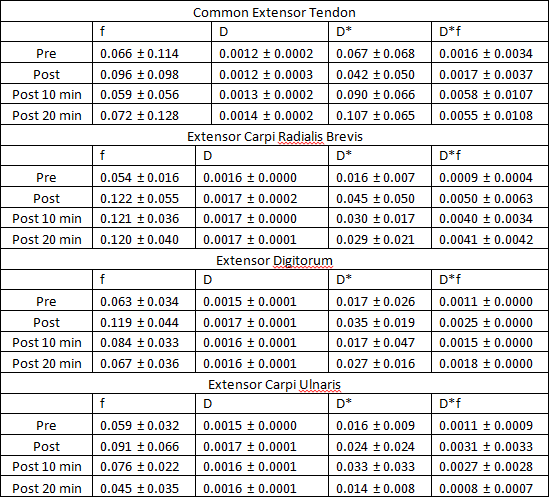
IVIM Parameters derived from various ROIs
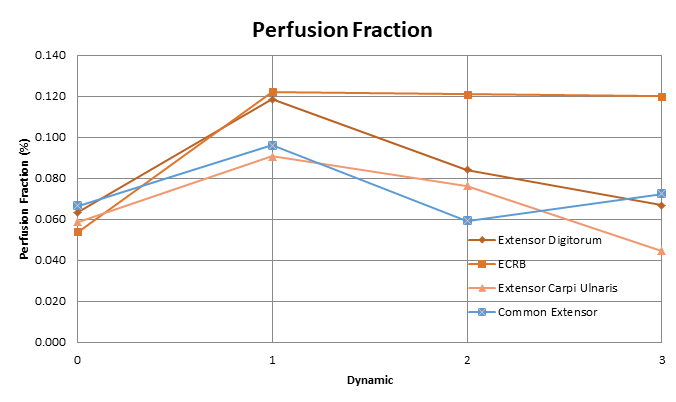
Perfusion Fraction
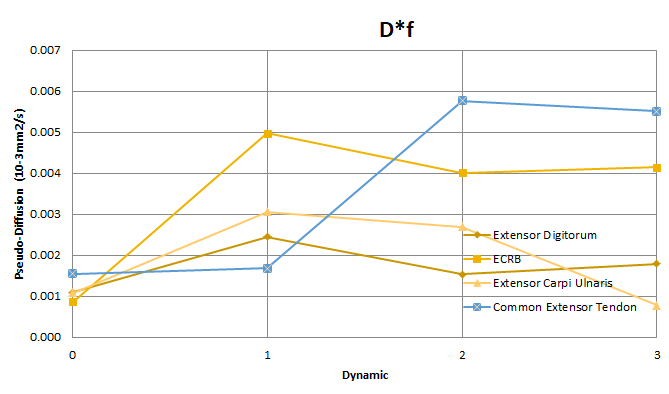
Diffusion Fraction * Perfusion Fraction
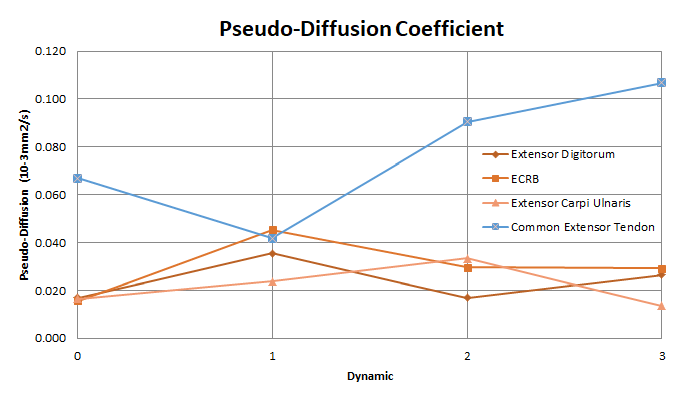
Pseudo-Diffusion Coefficient