5184
Super-resolution Reconstruction of Knee MRI1Dept. of Radiology, Antwerp University Hospital and University of Antwerp, Antwerp, Belgium, 2Imec/Vision Lab, Dept. of Physics, University of Antwerp, Antwerp, Belgium
Synopsis
Clinical knee MRI is most commonly performed with 2D-turbo-spin-echo (TSE) sequences in multiple imaging planes. Although these multi-slice sequences provide excellent tissue contrast and high in-plane spatial resolution, they use relatively thick slices, which leads to partial volume effects. This study used super-resolution reconstruction (SRR) to reconstruct isotropic high-resolution knee MR images. Our results indicate that SRR of knee MRI is feasible and compares favorably to direct high-resolution TSE acquisition in terms of image quality and acquisition time. SRR provides an attractive alternative for isotropic 3D-MRI of the knee.
Introduction
Current knee MR protocols consist of 2D-turbo-spin-echo (TSE) sequences repeated in multiple imaging planes1. Although these sequences provide excellent tissue contrast and high in-plane resolution, their relatively thick slices cause partial volume averaging, with a concomitant loss in diagnostic accuracy.
Isotropic 3D-TSE sequences are clinically available. These sequences provide thin, contiguous slices through the joint, thereby reducing partial volume effects, and allowing to create multiplanar reconstructions2. However, due to poor image quality and blurring, which is a characteristic of 3D-TSE sequences due to their long echo-train, a single 3D-TSE acquisition cannot replace conventional 2D-TSE-sequences.
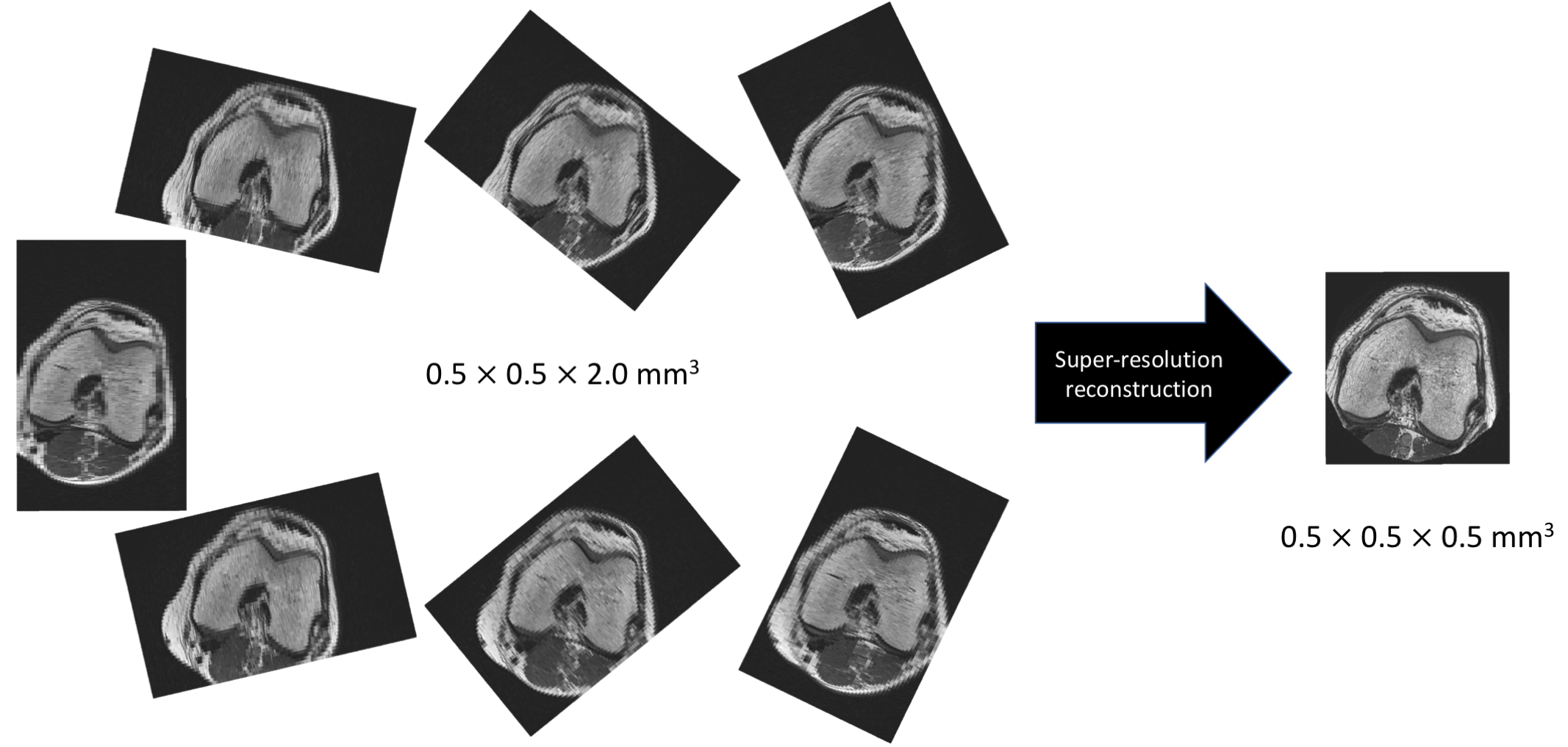
Super-resolution reconstruction (SRR) combines several distinct low-resolution observations of the same object into a single high-resolution image3. A SRR scheme in which low-resolution images are rotated around the phase encoding axis ensures that each low-resolution image covers a different part of k-space and thus adds information in the slice selection direction4 (Fig. 1). While SRR methods have been studied in MRI for different applications, most work has concentrated on brain MRI3-5. Our aim was to assess the feasibility of SRR for high-resolution MRI of the knee and to compare with direct 3D acquisition.
Methods
All examinations were performed on a 3T scanner (Magnetom PrismaFit, Siemens, Erlangen, Germany).
Super resolution reconstruction (SRR). The forward transformation from high-resolution images to low-resolution images with rotated slice stacks was performed efficiently using shear transformations6. The inverse operation (SRR) was solved as a linear least-squares problem with an additional total variation regularization term to improve the conditioning without losing fine details7.
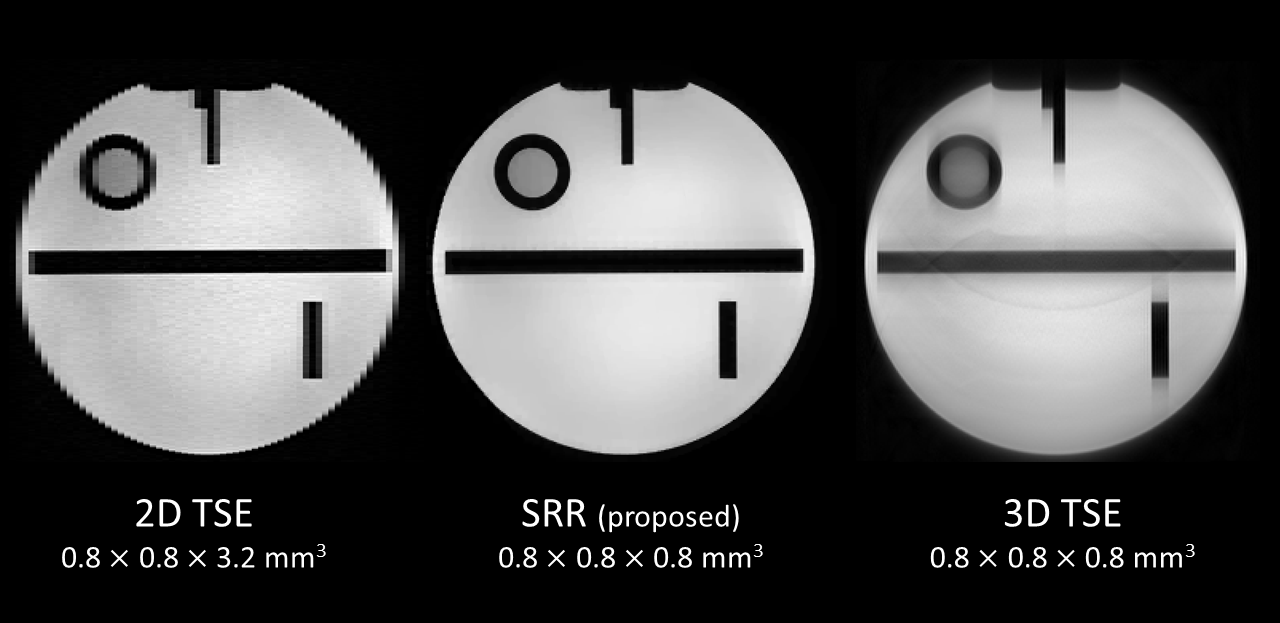
MRI phantom experiments. The ACR MRI Phantom (Newmatic Medical, MI, USA) was scanned using a 20-channel head coil. Imaging parameters of 2D-TSE sequence: TR/TE=4080/38 ms, FOV=205×205 mm2, matrix=256 × 256, slice thickness=3.2 mm, slice number=65, and a resolution of 0.8×0.8×3.2 mm3. The scan time per stack was 1min21s. The experiment was repeated 7 times, while the slice stack was rotated around the phase encoding direction in increments of approximately 26° (0°, 26°, 51°, 77°, 103°, 129°, 154°). SRR was performed to an isotropic high-resolution grid with voxel size 0.8×0.8×0.8 mm3. For comparison, direct 3D-TSE sequence was performed with matched scan time and resolution: TR/TE=1300/40 ms, FOV=205×205 mm2, matrix=256×256, slice thickness=0.8 mm, slice number=256, resolution of 0.8×0.8×0.8mm3, and scan time of 9min45s. Visual assessment of image quality and artifacts (blurring, discrimination from neighboring structures, signal homogeneity) was performed.
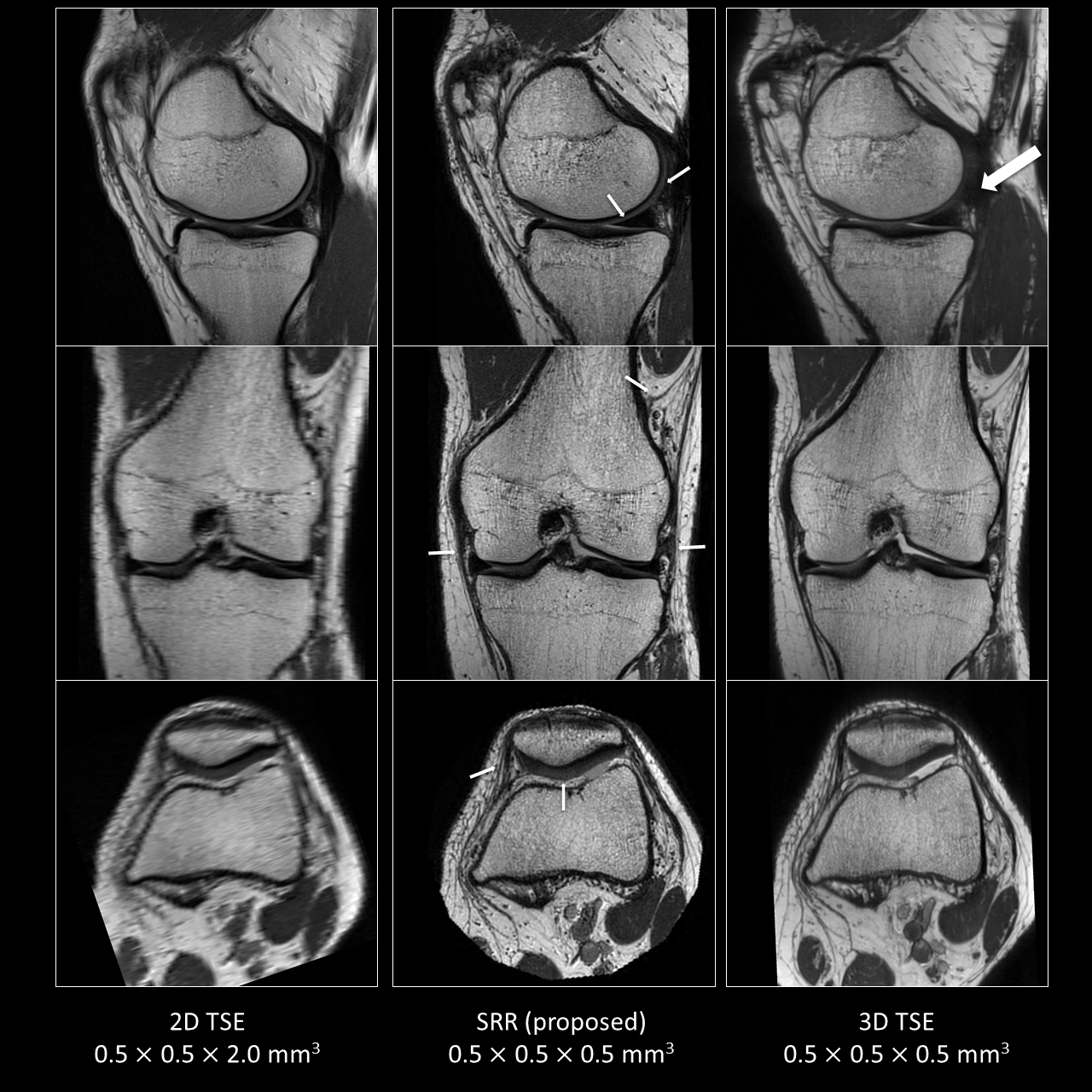
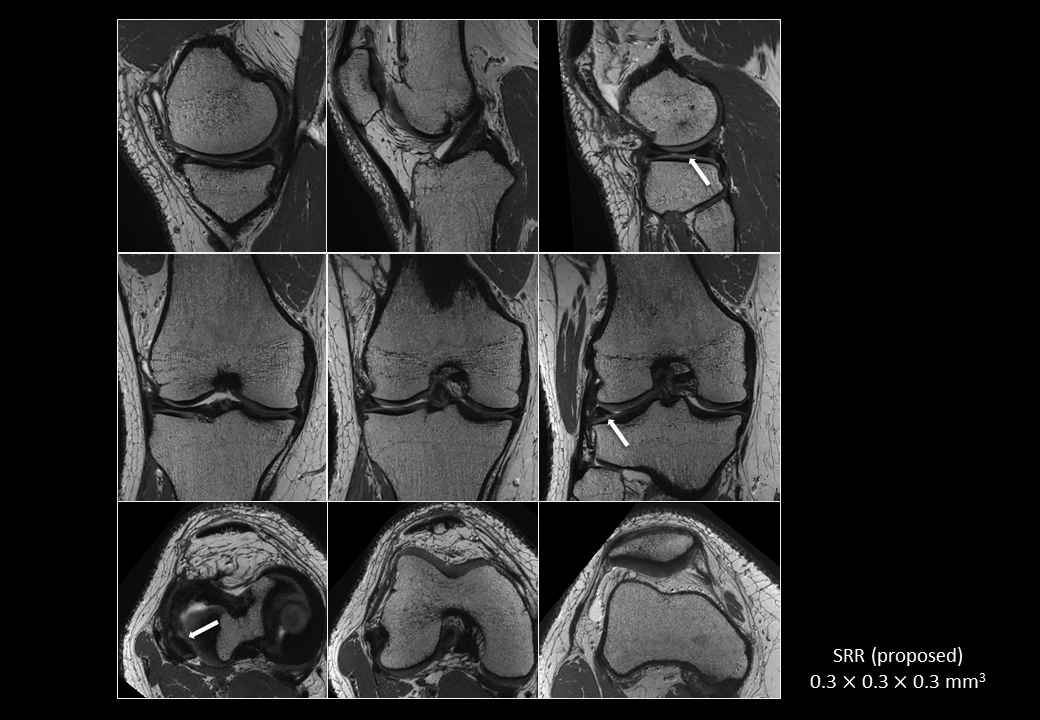
In vivo experiments. Imaging was performed on one volunteer and one patient using a 15-channel knee coil. Imaging parameters of 2D-TSE sequence: TR/TE=3080/36 ms, FOV 160×160 mm2, matrix=320×320, slice thickness=2 mm, slice number=53, and a resolution of 0.5×0.5×2.0 mm3. The scan time per stack was 1min55s. The experiment was repeated 7 times, with the same slice stack rotations as for the phantom experiments. SRR was performed to an isotropic high-resolution grid with voxel size 0.5×0.5×0.5 mm3. For comparison, direct 3D-TSE sequence was performed with matched scan time and resolution: TR/TE=1300/38 ms, FOV 160×160 mm2, matrix=320×320, slice thickness=0.5mm, slice number=208, resolution of 0.5×0.5×0.5 mm3, and scan time of 12min42s. To surpass the spatial resolution that can be obtained with currently available 3D sequences, another patient was scanned using 2D-TSE sequence with a resolution of 0.3×0.3×1.2 mm3. The scan time per stack was 8min55 s. The experiment was repeated 7 times, with the same slice stack rotations as for the previous experiments. SRR was performed to an isotropic high-resolution grid with voxel size 0.3×0.3×0.3 mm3. The depiction quality of normal and abnormal structures (menisci, cartilage, ligaments) was visually assessed.
Results
MRI phantom study. Fig. 2 shows 2D-TSE, SRR and direct 3D-TSE images of the phantom data. A clear improvement is seen from the low-resolution 2D-TSE image to the SRR result. Image blurring and ghosting-artifacts, and poor low-contrast object detectability is observed with direct 3D acquisition.
In vivo study. Fig. 3 shows a clear improvement in resolution achievable by SRR compared to the reference anisotropic low-resolution 2D-TSE images in a healthy volunteer. SRR also provides superior delineation of normal knee structures compared with direct 3D acquisition. Fig. 4 shows better depiction of abnormalities with SRR compared to direct 3D acquisition in a patient. Fig. 5 shows SRR image with 0.3×0.3×0.3 mm3 resolution. Although the acquisition time was long, this result significantly surpasses the resolution of that currently attainable with direct 3D acquisition for clinical knee imaging.
Conclusion
We demonstrate SRR of knee MRI is feasible and represents a valuable alternative to direct high-resolution acquisition for isotropic 3D imaging of the knee. Further improvement of time-efficiency can be expected with the use of simultaneous multi-slice (SMS) technique.Acknowledgements
PVD is a senior clinical investigator of the Research Foundation Flanders Belgium (FWO: 1831217N). BJ is a postdoctoral fellow of the Research Foundation Flanders Belgium (FWO: 12M3116N).References
1. Farjoodi P, Mesfin A, Carrino JA, Khanna AJ. Magnetic resonance imaging of the musculoskeletal system: basic science, pulse sequences, and a systematic approach to image interpretation. J Bone Joint Surg Am. 2010;92(Suppl 2):105-116.
2. Jung JY, Yoon YC, Kwon JW, Ahn JH, Choe BK. Diagnosis of internal derangement of the knee at 3.0-T MR imaging: 3D isotropic intermediate-weighted versus 2D sequences. Radiology. 2009;253(3):780-787.
3. Plenge E, Poot DH, Bernsen M, et al. Super-resolution methods in MRI: can they improve the trade-off between resolution, signal-to-noise ratio, and acquisition time? Magn Reson Med. 2012;68(6):1983-1993.
4. Shilling RZ, Robbie TQ, Bailloeul T, et al. A super-resolution framework for 3-D high-resolution and high-contrast imaging using 2-D multislice MRI. IEEE Trans Med Imaging. 2009;28(5):633-644.
5. Van Steenkiste G, Jeurissen B, Veraart J, et al. Super-resolution reconstruction of diffusion parameters from diffusion-weighted images with different slice orientations. Magn Reson Med. 2016;75(1):181-195.
6. Poot DH, Van Meir V, Sijbers J. General and efficient super-resolution method for multi-slice MRI. Med Image Comput Comput Assist Interv. 2010;13(Pt 1):615-622.
7. Barbero A, Sra S. Fast Newton-type methods for total variation regularization. In Proceedings of the 28th International Conference on Machine Learning (ICML-11), 2011, pp. 313-320.
Figures