5179
Usefulness of non-contrast perfusion using arterial spin labeling (ASL) for the differential diagnosis of shoulder pain1Radiology, Tobata General Hospital, Kitakyushu, Japan, 2Radiology, Sakura Clinic, Kitakyushu, Japan, 3Radiology, Mihagino Hospital, Kitakyushu, Japan, 4Radiology, Tobata Kyoritsu Hospital, Kitakyushu, Japan, 5Toshiba Medical Systems, Kasuga, Japan, 6Radiology, UC San Diego, La Jolla, CA, United States
Synopsis
We evaluated the usefulness of non-contrast perfusion obtained using arterial spin labeling (ASL) for the assessment and the differential diagnosis of shoulder disorders. Twenty consecutive patients were divided into 4 groups. Group 1 (partial tear or less) had no enhancement at the subacromional region; whereas, group 2 (full thickness tear of rotator cuff) showed significant enhancement due to bursitis. Group 3 (calcific tendinitis) and group 4 (osteoarthritis) also showed well enhancement. ASL perfusion could provide the additional physiological information to the morphological routine shoulder MRI without use of contrast materials, which is valuable for the management of shoulder disorders.
INTRODUCTION
Disorders of the rotator cuff tendons (RC) due to wear or tear are the most common causes of shoulder pain and disability. Magnetic resonance arthrography (MRA) has reported the superior diagnostic ability especially in partial RC tear and superior labrum anterior-to-posterior (SLAP) tears to conventional MRI (1); however, MRA is invasive because of direct injection of contrast media into the joint.
Arterial spin labeling (ASL) is now widely used for cerebral non-contrast perfusion examinations, which employ the labelled arterial blood by an inversion recovery (IR) pulse as endogenous contrast materials.
The purpose of this study is to evaluate the efficacy of non-contrast perfusion using an asymmetric slab STAR (ASTAR) method (2), one of pulsed ASL techniques, for the assessment and the differential diagnosis of shoulder disorders, especially RC tears.
MATERIALS and METHODS
A total of 20 consecutive patients (12 men and 8 women [17 – 82 y.o., mean, 63.5 y.o.]) underwent routine shoulder MRI was involved in this study. The final diagnoses of the cases were degeneration of RC of 3, partial tear of RC of 3, full thickness tear of RC of 10 (small 2, medium 2, large 4, and extensive 2), calcific tendinitis of 1, severe osteoarthritis (OA) of 1, and acromioclavicular (AC) arthritis of 2.
The patients were divided into 4 groups; group 1 included normal to degenerative changes of RC and partial tear of RC; group 2, full thickness tear of RC, (which subdivided into group 2a, small tear, and group 2b, medium, large, and extensive tear); group 3, calcific tendinitis; and group 4, OA. All patients underwent the ASTAR perfusion study of shoulder joint as well as routine shoulder MRI examinations.
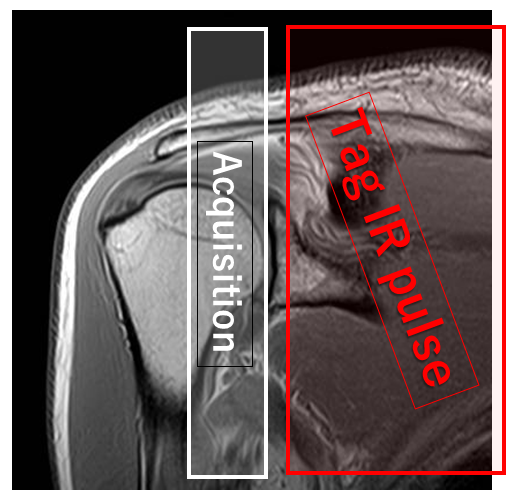
All MR examinations were performed using a 1.5-T clinical imager (EXCELART Vantage; Toshiba Medical, Tochigi, Japan) using a shoulder array 4ch coil. ASL was performed using the ASTAR 2 version. Fast field echo acquisition parameters were as follows: TR=9.0 msec, TE=3.6 msec, FA=15 degree, TI=1500 msec, matrix=64 x 64, section thickness=10 mm, FOV=15 x 15 cm, and the acquisition time of 2.5 minutes. Tag end cut (TEC)=2 (TEC TI1=400ms, TEC TI2=600ms) and control position=on were applied. The acquisition slice was placed longitudinally on the humeral head, including rotator cuff, subacromional bursa, inferior glenohumeral ligament, and acromioclavicular joint. Tag IR of a 30.0-mm thickness was placed on the subclavian artery (Fig.1).
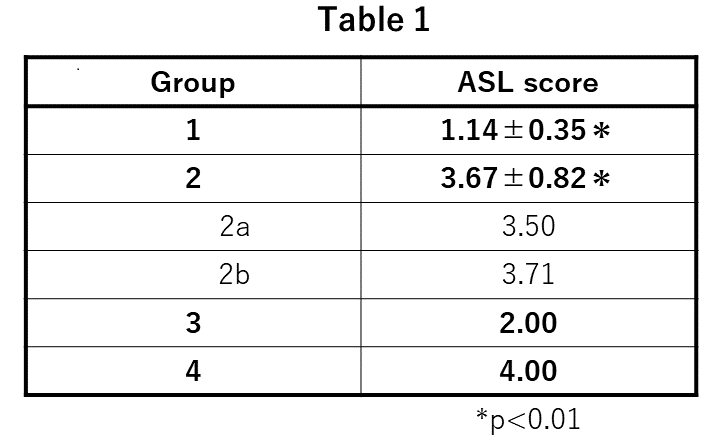
The ASL perfusion was evaluated by consensus reading with two observers regarding the degree of enhancement at the subacromional region using a five-point scoring system; score 1 was no enhancement; score 2, mild; score 3, moderate; score 4, severe; and score 5, extreme enhancement. The ASL score was compared with the hyperintensity of subacromional bursa in fat-suppressed T2WI. AC joint enhancement was also evaluated, which was compared with the hyperintensity of AC joint in fat-suppressed T2WI. Wilcoxon signed-rank test and Spearman's rank correlation coefficient were used for statistical analysis.
RESULTS
ASL score of group 2 was significantly higher than that of group 1, 3.67±0.82, 1.14±0.35, respectively (p<0.01) (Table 1). Groups 2a and 2b showed no significant difference. Groups 3 and 4 also showed high score. ASL score was well correlated with the hyperintensity of the subacromional bursa(correlation efficient = 0.730, p<0.01). The enhancement of AC joint was well correlated with the degree of osteoarthritis of AC joint (correlation efficient = 0.685, p<0.01).DISCUSSION
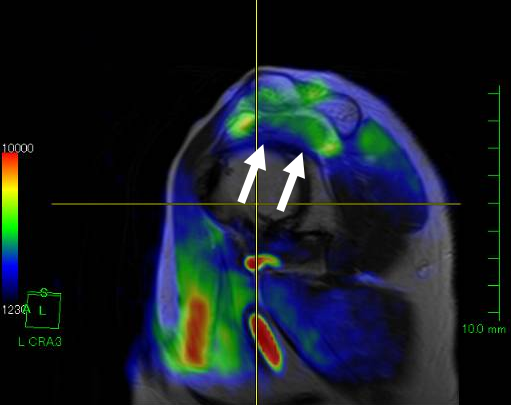
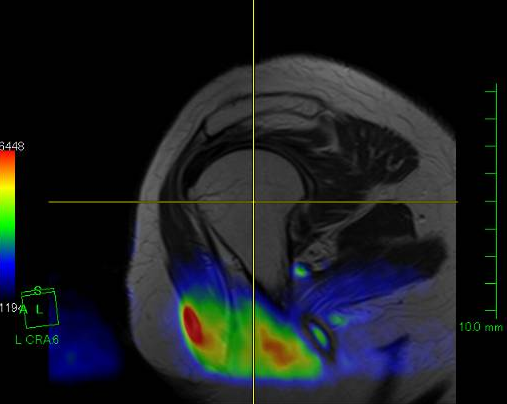
Because the continuity of rotator cuff is preserved in group 1, inflammatory stimuli to the shoulder bursae would be mild. On the contrary, the joint space communicates with subacromional bursa in the case of full thickness tear (group 2), which could set up the bursitis, then blood flow would increase at the site of inflammation. ASL score showed high in calcific tendinitis (group 3) and severe OA (group 4), which are known to trigger the inflammatory reaction around shoulder (3). Two of 5 cases of normal or the degenerative changes of RC showed the enhancement of AC joint, which then diagnosed as the arthritis of AC joint. ASL perfusion seems useful for the detection of AC joint disease, because the abnormalities of AC joint might be overlooked.CONCLUSION
ASL perfusion results clearly differentiated the full thickness tear of the rotator cuff from the partial thickness tear or degeneration of RC. ASL perfusion could provide the additional physiological information to the morphological routine shoulder MRI without use of contrast materials, which must be valuable for the management of the shoulder disorders.Acknowledgements
No acknowledgement found.References
1. Magee T. 3-T MRI of the shoulder: is MR arthrography necessary? AJR Am J Roentgenol. 2009 Jan;192(1):86-92.
2. Tokunori Kimura; Non-invasive perfusion imaging by modified STAR using asymmetric inversion slabs (ASTAR). Japanese Journal of Magnetic Resonance in Medicine; 20(8); 374-385c, 2000
3. Hackett L, Millar NL, Lam P, Murrell GA. Are the Symptoms of Calcific Tendinitis Due to Neoinnervation and/or Neovascularization? J Bone Joint Surg Am. 2016 Feb 3;98(3):186-92.
Figures