5178
Pre-operative MRI for Predicting Clinical Outcome Following Rotator Cuff Tendon Repair Surgery1Department of Radiology, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
This study was performed to determine whether pre-operative MRI could provide prognostic information regarding clinical outcome following rotator cuff tendon repair surgery. The study group consisted of 141 patients undergoing surgical repair of a full-thickness rotator cuff tendon tear who completed the Disabilities of Arm, Shoulder and Hand (DASH) and Short Form (SF-12) surveys before and one year after surgery. The pre-operative MRI was reviewed to determine tear size, tear retraction, torn tendon tendinosis, and composite muscle atrophy. There was a significant inverse association (p<0.05) between post-operative DASH and SF-12 scores and tear width, tendon retraction, and torn tendon tendinosis.
Introduction
This study was performed to determine whether pre-operative magnetic resonance imaging (MRI) could provide prognostic information regarding clinical outcome following rotator cuff tendon repair surgery.Methods
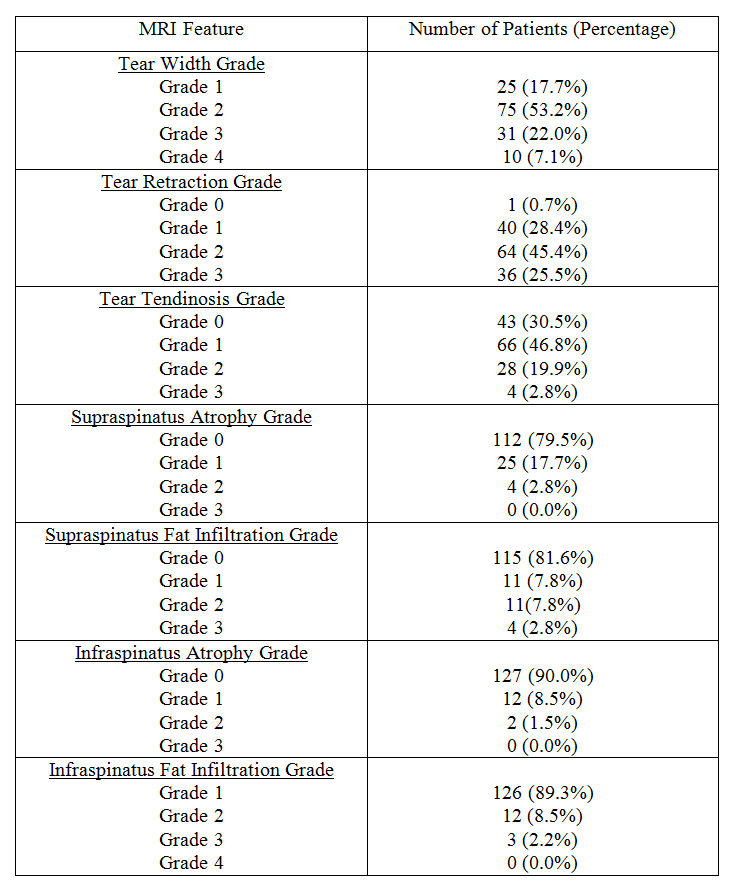
The study group consisted of 141 patients undergoing surgical repair of a full-thickness rotator cuff tendon tear who completed the upper extremity specific 11-item Disabilities of Arm, Shoulder and Hand survey (DASH) and generalized 12-item Short Form health survey (SF-12) prior to and one year following surgery. The SP-12 consisted of a composite physical component summary (PCS) score and scores for individual domains including physical function (PF) that evaluated the extent to which generalized health limited performance of physical activities, role-physical (RP) that evaluated the extent to which generalized health limited the quality and efficiency of performance of physical activities, and bodily pain (BP) that evaluated overall pain severity. All patients underwent a pre-operative MRI examination of the shoulder performed on a 1.5T or 3T scanner (Signa HdX, GE Healthcare, Waukesha, WI) which included sagittal-oblique and coronal-oblique T1-weighted and fat-suppressed T2-weighted fast spin-echo sequences. The MRI examinations of all patients were retrospectively reviewed by a musculoskeletal radiologist blinded to the clinical findings to assess the following categorical features of the torn rotator cuff tendon: tear width [1], tear retraction [2], torn tendon tendinosis [3, 4], and composite muscle atrophy which took into account the degree of atrophy [5] and fat infiltration [6] of the supraspinatus and infraspinatus muscles. The radiologist also measured the maximal anterior-posterior width and medial-lateral retraction of the torn rotator cuff tendon using electronic calibers on the imaging work-station. Multi-variate linear regression models were used to determine the association between post-operative DASH and SP-12 scores and MRI features of the torn rotator cuff tendon adjusted for age, gender, surgeon, and pre-operative DASH and SP-12 scores with the Holt-Bonferroni method used to account for analysis of multiple variables.Results
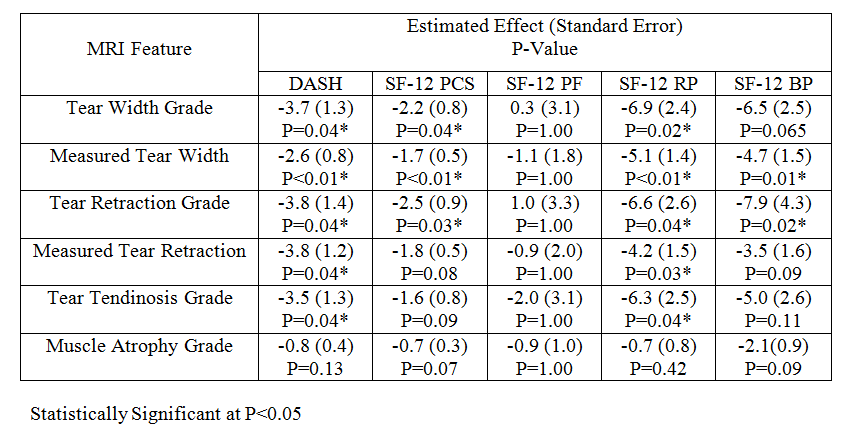
The mean pre-operative, post-operative, and change for the DASH and SF-12 scores are shown in Table 1. One-hundred thirty-five (95.7%), 132 (93.6%), 113 (80.1%), 124 (87.9%), and 123 (87.2%) patients showed an increase in DASH, PCS, PF, RP, and BP scores respectively following surgery indicating clinical improvement. The distribution of categorical MRI features of the torn rotator cuff tendon is summarized in Table 2. The mean maximum anterior-posterior width and medial-lateral retraction of the rotator cuff tendon tear were 2.6cm (1.4cm standard deviation) and 2.2cm (1.3cm standard deviation) respectively. As shown in Table 3, there was a significant inverse association (p<0.05) between the post-operative DASH, PCS, RP, and BP scores and tear width and tendon retraction with the association being the strongest for the DASH and RP scores where statistical significance was present for both categorical and continuous variables. There was also a significant inverse association (p<0.05) between the post-operative DASH and RP scores and torn tendon tendinosis. There was no significant association between PF score and MRI features (p=1.00) or between DASH and SF-12 scores and composite muscle atrophy (p=0.07-0.42).Discussion
The vast majority of patients undergoing rotator cuff tendon repair surgery showed clinical improvement one year following surgery. However, there was a significant inverse association between the post-operative DASH and RP scores and tear width, tendon retraction, and torn tendon tendinosis. When comparing the individual domains of the SF-12 survey, there was a significant inverse association between MRI features and RP score but not PF score indicating that patients with larger, more retracted tears could perform the same physical activities as patients with smaller, less retracted tears following surgery, but they did not perform these activities as well or as efficiently. Multiple previous studies found no significant association between clinical outcome scores and tear size measured at surgery [7-11], while one previous study found a significant inverse correlation between clinical outcome score and tear size measured on pre-operative MRI [12]. No previous studies have investigated the association between clinical outcome scores and tendon retraction or torn tendon tendinosis. Multiple previous studies found a significant inverse association between clinical outcome scores and rotator cuff muscle atrophy and fat infiltration [6, 7, 12] which was not documented in our study. This may be the result of the small number of patients with rotator cuff tears and moderate or severe rotator cuff muscle atrophy and fat infiltration which is likely due to improvements in surgical candidate selection at our institution based upon the findings of previous studies.Conclusion
Pre-operative MRI features including tear width, tendon retraction, and torn tendon tendinosis can provide prognostic information regarding clinical outcome following rotator cuff tendon repair surgery.Acknowledgements
We acknowledge support from NIH R01-AR068373-01, GE Healthcare, and University of Wisconsin Department of Radiology Research and Development Committee.References
[1] J.K. DeOrio, R.H. Cofield, Results of a second attempt at surgical repair of a failed initial rotator-cuff repair, The Journal of bone and joint surgery. American volume, 66 (1984) 563-567.
[2] D. Patte, Classification of Rotator Cuff Lesions, Clinical orthopaedics and related research, (1990) 81-86.
[3] S.W. Chung, J.Y. Kim, J.P. Yoon, S.H. Lyu, S.M. Rhee, S.B. Oh, Arthroscopic repair of partial-thickness and small full-thickness rotator cuff tears: tendon quality as a prognostic factor for repair integrity, The American journal of sports medicine, 43 (2015) 588-596.
[4] M.L. Sein, J. Walton, J. Linklater, C. Harris, T. Dugal, R. Appleyard, B. Kirkbride, D. Kuah, G.A. Murrell, Reliability of MRI assessment of supraspinatus tendinopathy, British journal of sports medicine, 41 (2007) e9.
[5] J.J. Warner, L. Higgins, I.M.t. Parsons, P. Dowdy, Diagnosis and treatment of anterosuperior rotator cuff tears, Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et al.], 10 (2001) 37-46.
[6] D. Goutallier, J.M. Postel, J. Bernageau, L. Lavau, M.C. Voisin, Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan, Clinical orthopaedics and related research, (1994) 78-83.
[7] J.N. Gladstone, J.Y. Bishop, I.K. Lo, E.L. Flatow, Fatty infiltration and atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with poor functional outcome, The American journal of sports medicine, 35 (2007) 719-728.
[8] L.V. Gulotta, S.J. Nho, C.C. Dodson, R.S. Adler, D.W. Altchek, J.D. MacGillivray, H.S.S.A.R.C. Registry, Prospective evaluation of arthroscopic rotator cuff repairs at 5 years: part II--prognostic factors for clinical and radiographic outcomes, Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et al.], 20 (2011) 941-946.
[9] R. Kluger, P. Bock, M. Mittlbock, W. Krampla, A. Engel, Long-term survivorship of rotator cuff repairs using ultrasound and magnetic resonance imaging analysis, The American journal of sports medicine, 39 (2011) 2071-2081.
[10] L. Lafosse, R. Brozska, B. Toussaint, R. Gobezie, The outcome and structural integrity of arthroscopic rotator cuff repair with use of the double-row suture anchor technique, The Journal of bone and joint surgery. American volume, 89 (2007) 1533-1541.
[11] S.J. Nho, B.S. Brown, S. Lyman, R.S. Adler, D.W. Altchek, J.D. MacGillivray, Prospective analysis of arthroscopic rotator cuff repair: prognostic factors affecting clinical and ultrasound outcome, Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et al.], 18 (2009) 13-20.
[12] J.M. Mellado, J. Calmet, M. Olona, C. Esteve, A. Camins, L. Perez Del Palomar, J. Gine, A. Sauri, Surgically repaired massive rotator cuff tears: MRI of tendon integrity, muscle fatty degeneration, and muscle atrophy correlated with intraoperative and clinical findings, AJR. American journal of roentgenology, 184 (2005) 1456-1463.
Figures