5145
Diffusion tensor imaging of the human calf in healthy and diseased subjects during plantar-flexion exercise1Washington University School of Medicine in St. Louis, St. Louis, MO, United States
Synopsis
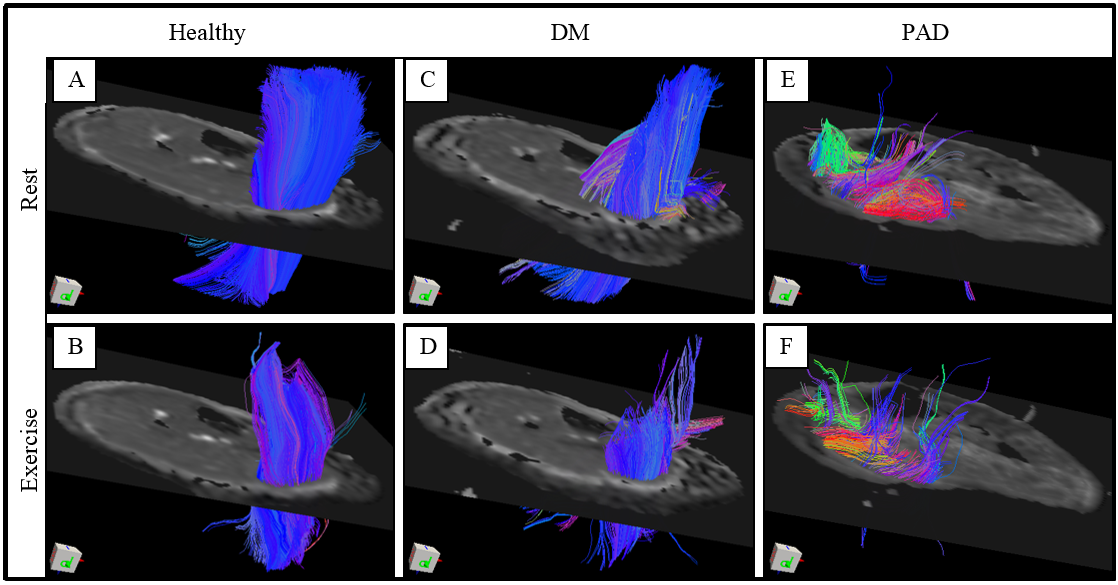
This study aims to elucidate diffusion variations between human healthy and diseased calf muscles. Subjects were assigned into three groups: healthy, diabetes mellitus (DM), and peripheral artery disease (PAD). DTI echo planar imaging was performed at rest and ankle plantar-flexion to provide fractional anisotropy (FA), mean diffusivity (MD), and fiber length for calf medial gastrocnemius (MG), lateral gastrocnemius (LG), and soleus (SOL). Our initial results revealed noticeable diffusion indices variations from resting to contraction of the above muscles between healthy and diseased groups and demonstrated a good accordance with previous healthy studies in the literature.
Purpose
DTI has been widely used to noninvasively evaluate and characterize in vivo skeletal muscle structure and pathology 1-2. There are many studies indicating the potential and capability of DTI to reveal the human calf muscle architecture 3-4-5. However, calf DTI studies have been explored diffusion properties during muscle contraction only in healthy subjects or in injured calf muscle at resting state 6-7-8. This project aims to assess diffusion differences during rest and ankle plantar-flexion in healthy compared to patients with DM and PAD.Methods
Twenty subjects were recruited and examined in a 3T whole-body MRI scanner after obtaining consents. Subjects were assigned in three groups as follows: healthy (n=5; age: 57.40±12.52y; weight: 111.22±18.95kg), DM (n=11; age: 65.09±10.69y; weight: 90.60±17.44kg), and PAD (n=4; age: 65.75±9.50y; weight: 88.76±19.93kg). A custom-made MRI compatible device was built consisting a pedal with adjusting pressure gauge (pedal stopper initially set to 10 psi) that was attached to a base plate where it resembles a foot brake. For rest scan, subjects laid in foot/supine position; for flexion exercise, they were asked to press the pedal until it reaches the stopper and hold it steadily during scan. DTI parameters were optimized for calf imaging to acquire a series of axial slices: TR/TE= 4500/70 ms, 20 slices, matrix size 192×144, spatial resolution 1.14×1.14 mm2, slice thickness 6 mm, NEX= 4, 12 gradient directions for b-values of 0 and 500 s/mm2. DTI acquisition time was approximately 4min. DTI were successfully obtained from all subjects with sufficient quality. All DTI images were registered to non-diffusion image (b=0) and corrected for motion, diffusion gradient table, and eddy current distortion using MATLAB and DSI Studio.
Results
Table 1 shows DTI results during the flexion exercise. The healthy results were in a good agreement with previous reports 3-6-7-8. From rest (data not shown here) to flexion exercise, FA showed decreases in MG, LG, and SOL muscles for patient groups, whereas the largest reduction in FA were seen in the healthy group (p<.05). Among all muscles, mean MD increased between rest and exercise in both patient groups with the significant difference in the DM group (p<.05), but the healthy group showed the least increase in MD.
Progressive increasing trend of FA and MD across all muscle groups were observed from healthy to DM and PAD (Table 1) during plantar-flexion exercise, except MD in LG muscle of the DM group. Significant differences in FA and MD between healthy and PAD during exercise were observed in LG and SOL muscles, respectively (p<.05). Healthy fiber length between rest and flexion were showed ~32% mean reduction for MG, LG, SOL (p<.05). DM group showed slightly greater fiber length shortening (~36%, p<.05) (Figure 1). Although fiber length reduction were also observed in MG, and SOL muscles within PAD group, they were not statistically significant except for LG muscle.
Discussion
It is well understood that the skeletal muscle impairment alters muscle microstructure integrity, subsequently leads to changes in diffusion properties such as anisotropy, diffusivity, and fiber arrangements. We, for the first time, demonstrated differences in diffusion properties in healthy and diseased calf muscles between rest and exercise, as well as between healthy and patients with DM or PAD. Healthy group showed lower FA and MD values comparing to diseased groups while FA reduction and MD elevation were observed from rest to exercise. While FA and MD showed similar changes in DM and PAD groups, fiber length changes appeared more in DM than that in PAD. It suggests that the severity of microstructure dysfunction may be equal to or greater in DM compared to PAD. This initial study demonstrated promising potential to promote DTI as an established technique for noninvasive clinical evaluation of muscle microstructure in patients with microcirculation dysfunction, such as DM and PAD.Acknowledgements
No acknowledgement found.References
1. Heemskerk AM, Damon BM. Diffusion Tensor MRI Assessment of Skeletal Muscle Architecture. Current medical imaging reviews. 2007; 3(3):152-160. doi:10.2174/157340507781386988.
2. Schlaffke, L., Rehmann, R., Froeling, M., Kley, R., Tegenthoff, M., Vorgerd, M. and Schmidt-Wilcke, T. Diffusion tensor imaging of the human calf: Variation of inter- and intramuscle-specific diffusion parameters. J. Magn. Reson. Imaging. 2017; 46: 1137–1148. doi:10.1002/jmri.25650.
3. Saupe N, White LM, Sussman MS, Kassner A, Tomlinson G, Noseworthy MD. Diffusion tensor magnetic resonance imaging of the human calf: comparison between 1.5 T and 3.0 T-preliminary results. Invest Radiol. 2008; 43(9):612-8.
4. Galban CJ, Maderwald S, Uffmann K, et al. Diffusive sensitivity to muscle architecture: a magnetic resonance diffusion tensor imaging study of the human calf. Eur J Appl Physiol. 2004; 93:253–262.
5. Sinha S, Sinha U, Edgerton VR. In vivo diffusion tensor imaging of the human calf muscle. J Magn Reson Imaging. 2006; 24:182–190.
6. Deux JF, Malzy P, Paragios N, et al. Assessment of calf muscle con-traction by diffusion tensor imaging. Eur Radiol. 2008; 18:2303–2310.
7. Schwenzer, N. F., Steidle, G., Martirosian, P., Schraml, C., Springer, F., Claussen, C. D. and Schick, F. Diffusion tensor imaging of the human calf muscle: distinct changes in fractional anisotropy and mean diffusion due to passive muscle shortening and stretching. NMR Biomed. 2009; 22:1047–1053. doi:10.1002/nbm.1409.
8. Zaraiskaya, T.,
Kumbhare, D. and Noseworthy, M. D. Diffusion tensor imaging in evaluation of
human skeletal muscle injury. J. Magn. Reson. Imaging. 2006; 24: 402–408.
doi:10.1002/jmri.20651.
Figures