5078
Intravoxel Inchoerent Motion MRI to Evaluate Post-Occlusive Reactive Hyperemia in Calf MusclesAlfonso Mastropietro1, Simone Porcelli1, Marcello Cadioli2,3, Letizia Rasica1,4, Elisa Scalco1, Simonetta Gerevini3, Mauro Marzorati1, and Giovanna Rizzo1
1Institute of Bioimaging and Molecular Physiology, Consiglio Nazionale delle Ricerche, Segrate, Italy, 2Philips Healthcare, Monza, Italy, 3Department of Neuroradiology, Ospedale San Raffaele, Milano, Italy, 4Department of Biomedical Sciences for Health, Università degli Studi di Milano, Milano, Italy
Synopsis
The main goal of this study was to evaluate changes of IVIM parameters related to muscle perfusion changes occurring in the calf of healthy subjects before, during and after transitory ischemia of lower limb. MRI acquisitions were performed on 11 healthy volunteers on a 3T scanner. IVIM was performed on the right calf before, during and after arterial occlusion. A slight
Introduction
MRI offers non-invasive, valuable and feasible techniques to study muscle perfusion. This can be useful for a better understanding of the microcirculation in physiological and pathological conditions (e.g. peripheral arterial disease (PAD)). Among them Arterial Spin Labeling (ASL) has emerged as a promising tool. In fact, ASL was recently used to study muscle perfusion in healthy subjects during hyperemia1 and patients affected by PAD2,3. Despite of its usefulness, ASL has some important pitfalls (low Signal to Noise Ratio (SNR), dependence on the T1 decay of blood and requirement of a priori knowledge) and Intravoxel Incoherent Motion4 (IVIM) has been proposed as an alternative effective approach to assess the exercise-induced muscle perfusion changes5,6. IVIM offers the advantage of better SNR than ASL, even on low-field MR scanners, at the expense of time resolution, without the need of a priori knowledge. The main goal of this study was to evaluate changes of IVIM parameters related to muscle perfusion changes occurring in the calf of healthy subjects before, during and after transitory ischemia of lower limb.Methods
MRI acquisitions were performed on 11 healthy moderately trained volunteers (5 women and 6 men; age: 29±4). Gastrocnemius and soleus perfusion was assessed on the right calf before (REST), during (ISCHEMIA) and after (RECOVERY) the arterial occlusion via a pneumatic cuff secured around the thigh (pressure = 280 mmHg, duration 5 minutes). Image acquisition at baseline was performed during 1 minute before the occlusion. ISCHEMIA images were collected for 2 minutes before the cuff deflation. During RECOVERY images were acquired 1 and 2 minutes after the end of the occlusion (see figure 1 for the detailed protocol). MRI was performed on a 3.0 T scanner (Ingenia CX, Philips Healthcare) equipped with a 32 channels body coil. The IVIM experiments were based on a DWI sequence using single-shot echo-planar imaging (EPI) readout. Diffusion images were acquired using three orthogonal gradient directions with the following parameters: field of view = 160 ×160 ×100 mm; voxel size 2.5 × 2.5 mm; slice thickness 10 mm; slices 10; TR=1500 ms; TE = 48 ms; b values = 0, 10, 20, 50, 100, 200, 350, and 500 s/mm2; NSA = 4 (duration = 2 min 14 sec) or 2 (duration = 1 min 7 sec)Fat suppression was performed combining the spectrally selective adiabatic inversion recovery (SPAIR) technique with slice-selective gradient reversal (SSGR). Data were fitted using a voxel-based, 2-steps, segmented approach that was implemented in a custom-made Matlab routine (release 2016b, MathWorks, Natick, MA, USA). ROIs corresponding to the gastrocnemius and the soleus were manually delineated on b0 images. Differences in D, D*, f and f·D* among conditions (rest, ischemia, recovery1, recovery 2) were calculated using a non-parametric Friedman's test.Results
Figure 2 shows an example of ROIs drawn on gastrocnemius and soleus muscles overimposed to b0 image. Furthermore, IVIM parameters maps (diffusion D, perfusion fraction f, pseudodiffusion D* and perfusion related parameter fD*), calculated in a single subject, are displayed and compared in all the experimental phases. As to D, a significant increase was shown just during RECOVERY 1 with respect to REST and ISCHEMIA in both muscles. No significant differences were found in f during all phases. A slight reduction of D* and fD* was observed in the gastrocnemius during ischemia even if these changes were not significant. During RECOVERY 1, D* increased significantly in gastrocnemius whereas fD* significantly increased in both muscles during the hyperemia. During RECOVERY 2 an almost complete recovery of all parameters was observed. Figure 3 shows detailed results in all the subjects.Discussion
The slight reduction of D* and fD* observed during ISCHEMIA in gastrocnemius, even if not significant and not clearly shown at the same time in soleus, is in agreement with the results obtained by ASL in similar conditions. The significant increase of D*, fD* and D observed during hyperemia can be explained by the increased velocity of the blood flowing in the tissue and the consequent augmented muscle perfusion, as well as the increase of temperature occurring after the end of the occlusion. Within 2 minutes after the deflation, the perfusion related parameters recovered towards REST values in agreement with the physiologic transient hyperemic response and with previous findings obtained using ASL1.Conclusion
IVIM appears as a promising tool to evaluate muscle perfusion related parameters in hyperemia. Further studies and better interpretations of the model are needed in order to explain some controversial findings especially during ischemia.Acknowledgements
The work was partially supported by the Future Home for Future Communities (FHfFC) Project within the Framework Agreement between Regione Lombardia and National Research Council, D.G.R. n. 7884 – 05/08/2016 and by the project "EMpatia@Lecco" funded by Regione Lombardia and Fondazione Cariplo, call Emblematiche Maggiori 2016, Provincia di Lecco.References
- Englund EK, Rodgers ZB, Langham MC, Mohler ER, Floyd TF, Wehrli FW. Measurement of skeletal muscle perfusion dynamics with pseudo-continuous arterial spin labeling (pCASL): Assessment of relative labeling efficiency at rest and during hyperemia, and comparison to pulsed arterial spin labeling (PASL). J Magn Reson Imaging. 2016;44(4):929-939.
- Grözinger G, Pohmann R, Schick F, et al. Perfusion measurements of the calf in patients with peripheral arterial occlusive disease before and after percutaneous transluminal angioplasty using MR arterial spin labeling. J Magn Reson Imaging. 2014;40(4):980-987.
- Lopez D, Pollak AW, Meyer CH, et al. Arterial spin labeling perfusion cardiovascular magnetic resonance of the calf in peripheral arterial disease: cuff occlusion hyperemia vs exercise. J Cardiovasc Magn Reson. 2015;17(1):23.
- Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988;168(2):497-505.
- Filli L, Boss A, Wurnig MC, Kenkel D, Andreisek G, Guggenberger R. Dynamic intravoxel incoherent motion imaging of skeletal muscle at rest and after exercise. NMR Biomed. 2015;28(October 2014):240-246.
- Nguyen A, Ledoux J-B, Omoumi P, Becce F, Forget J, Federau C. Application of intravoxel incoherent motion perfusion imaging to shoulder muscles after a lift-off test of varying duration. NMR Biomed. 2016;29(1):66-73.
Figures
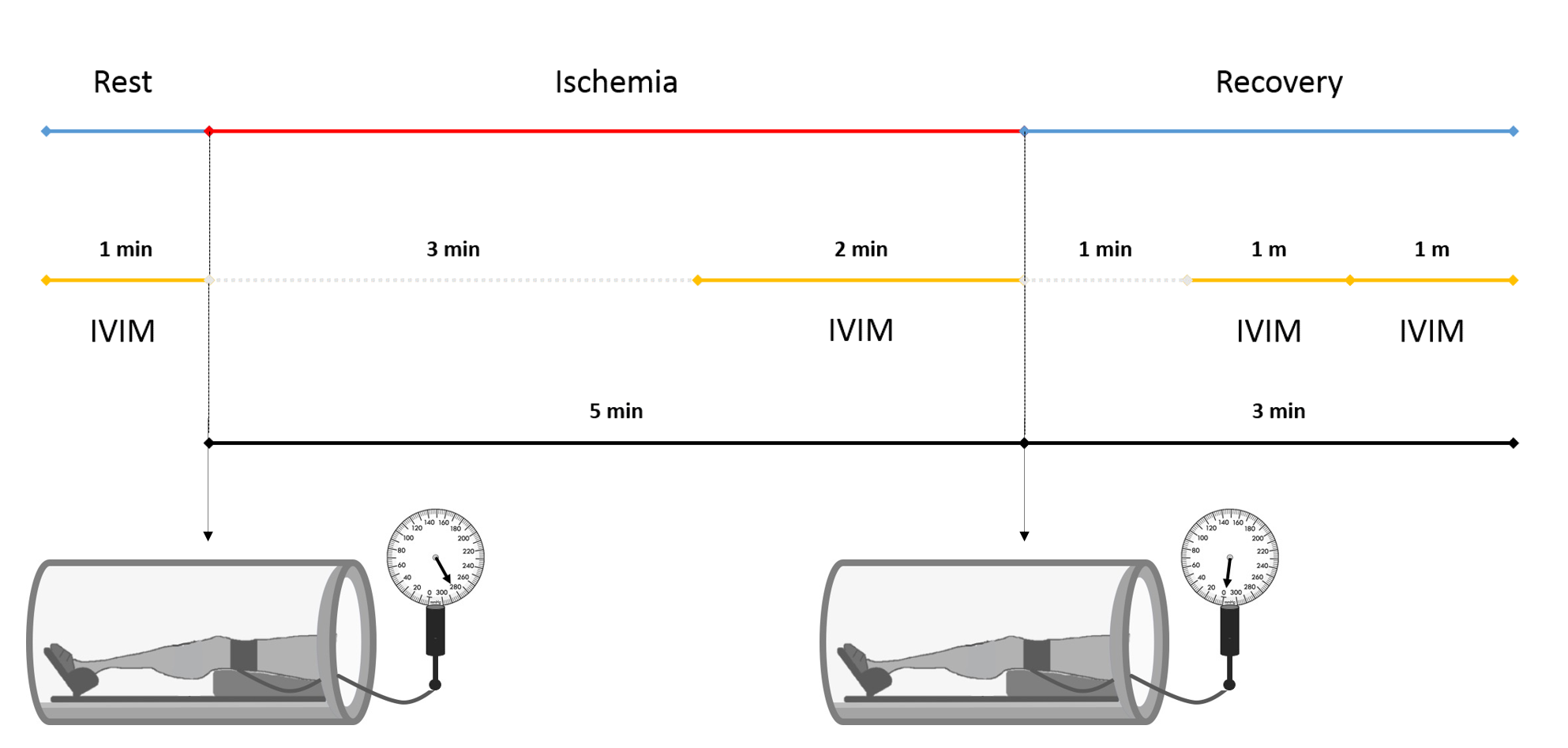
The whole protocol consisting of rest,
ischemia and recovery phases is schematically displayed.
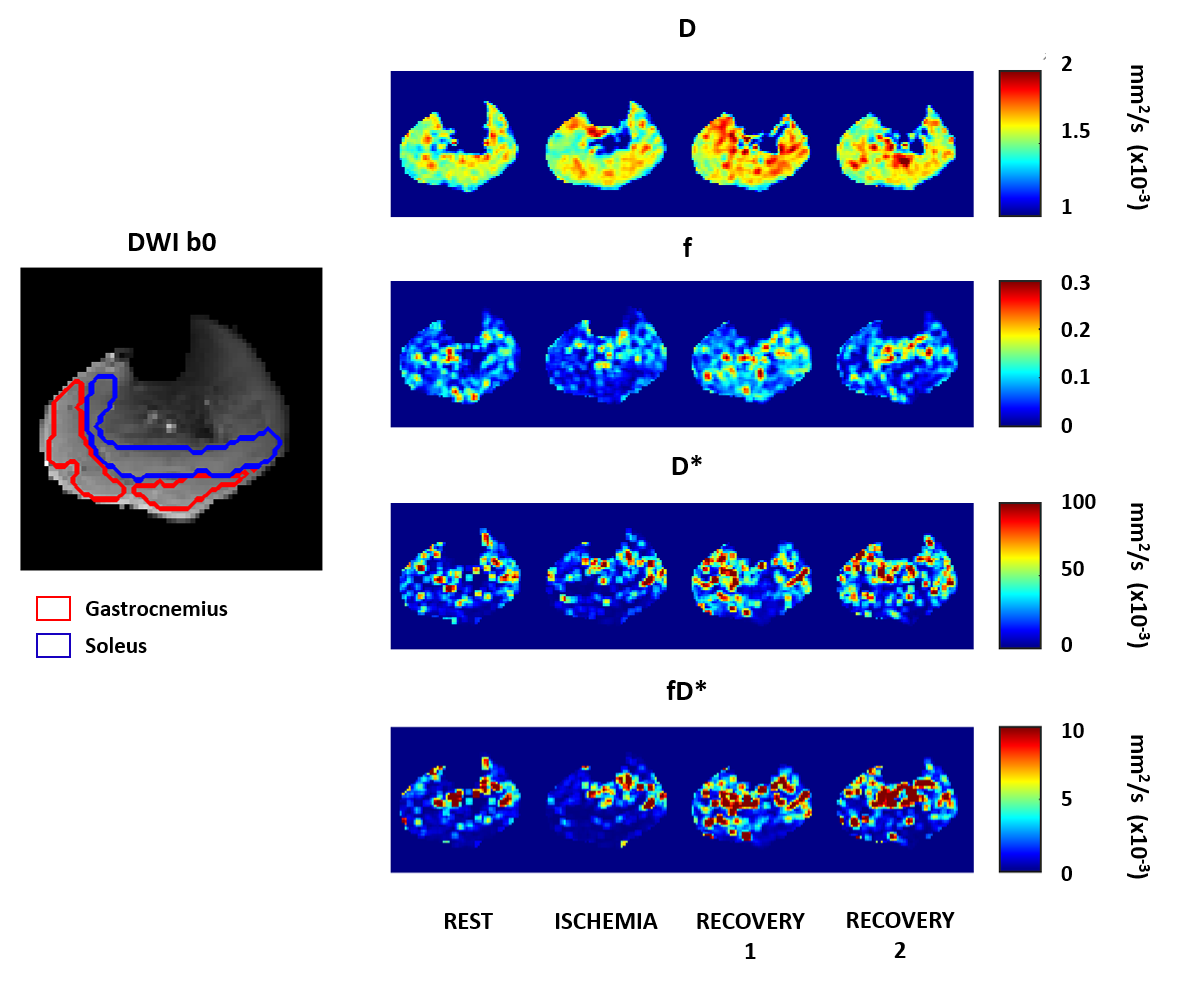
An example of IVIM parametrical maps of the calf muscles during rest, ischemia, early and late recovery phases. The ROIs depicted in the gastrocnemius and soleus muscles and superimposed to the corresponding b0 image are shown in the left panel.
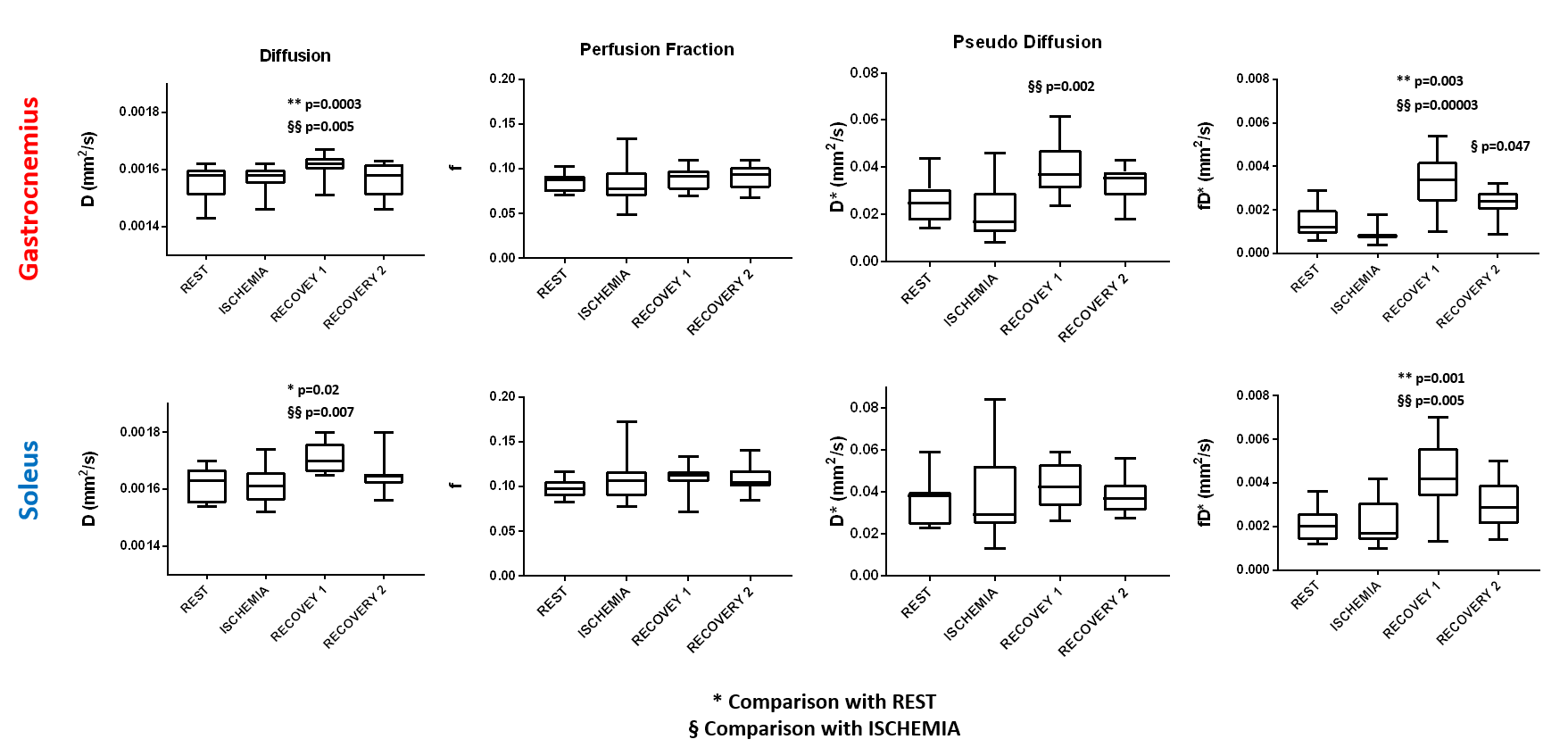
Changes of D, f, D* and fD* during the different phases of the protocol in the gastrocnemius and soleus muscles are displayed. * highlights significant differences with respect to rest whereas § refers to significant changes with respect to ischemia.