5074
Repeatability and Reproducibility of Diffusion Tensor MRI and 2-Point Dixon Fat Fraction Measurements in the Muscle1Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, United Kingdom, 2NIHR Leeds Biomedical Research Centre, Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom
Synopsis
Muscle deterioration is associated with fat infiltration and alterations in muscle
Introduction
Muscle health deteriorates due to age 1, muscle disease 2 and from corticosteroid use 3. This deterioration is often associated with fat infiltration and alterations in muscle fibre architecture 4. Muscle biopsies and manual muscle testing are frequently used assessment tools. However, muscle biopsies are invasive for the individual and manual muscle testing is subjective 5. Quantitative MRI measurements are of interest as evidence suggests they may be able to detect changes in muscle caused by disease and ageing 4. Fat fraction (FF) provides a quantitative measure of fat infiltration into muscles. Diffusion tensor imaging (DTI) measures water diffusion within tissues which is sensitive to changes in muscle microstructure. Before applying these techniques in research their repeatability and reproducibility should be established in order to assess their sensitivity. The existing literature on the repeatability and reproducibility of DTI and FF in skeletal muscles is sparse and uses small sample sizes 6, 7. The aim of this study was to evaluate the repeatability and reproducibility of quantitative measures of FF and DTI within the thigh muscles of healthy participants in a relatively large study involving 19 healthy volunteers.Methods
This study utilised STEAM-EPI diffusion and 2-point Dixon with a 3D gradient echo readout (VIBE) (Table 1). 19 participants had two examinations separated by a thirty-minute break when they were removed from the table. Mean diffusivity (MD), fractional anisotropy (FA) and eigenvalue parameter maps were generated. Regions of interest were contoured by two researchers. Regions depicting the individual muscles that make up the hamstring and quadriceps were drawn on the middle slice of the in-phase VIBE Dixon volume. These ROIs were copied on to the corresponding slice of the diffusion series. Mean hamstrings, quadriceps and whole thigh measurements were obtained by combining these ROIs. For test-retest repeatability, two MRI data sets were completed and marked by the same researcher. For intra-rater repeatability, the first MRI data set was contoured twice by the same researcher. For inter-rater reproducibility, the first MRI scan was contoured by two researchers. Repeatability and reproducibility was measured using the intraclass correlation coefficient (ICC). Agreement was measured using Bland Altman plots. For ICC, a two-way mixed model with absolute agreement was used. ICC values above 0.60 were classed as good and values above 0.75 classed as excellent reproducibility/repeatability between the two measurements 8.
Results
Figures 1-3 show that there is good agreement between measures with small biases. ICCs for test-retest repeatability, intra-rater repeatability and inter-rater reproducibility showed excellent repeatability and reproducibility (Table 2).
Discussion and Conclusion
This study found excellent repeatability and reproducibility for FF and DTI measurements with small differences between scans and observers. This implies that the measurements have sufficient precision to detect subtle changes. These techniques have the potential to be used to investigate changes in muscles in response to factors such as ageing, disease and treatments 9, 10.Acknowledgements
With thanks to the Leeds BRC radiographers.References
1. D. G. Candow and P. D. Chilibeck, 'Differences in size, strength, and power of upper and lower body muscle groups in young and older men', J Gerontol A Biol Sci Med Sci, 60 (2005): 148-56.
2. C. Ekdahl and G. Broman, 'Muscle strength, endurance, and aerobic capacity in rheumatoid arthritis: a comparative study with healthy subjects', Annals of the Rheumatic Diseases, 51 (1992): 35-40.
3. S. Perrot and C. Le Jeunne, '[Steroid-induced myopathy]', Presse medicale (Paris, France : 1983), 41 (2012): 422-426.
4. T. A. Willis, K. G. Hollingsworth, A. Coombs, M.-L. Sveen, S. Andersen, T. Stojkovic, M. Eagle, A. Mayhew, P. L. de Sousa, L. Dewar, J. M. Morrow, C. D. J. Sinclair, J. S. Thornton, K. Bushby, H. Lochmüller, M. G. Hanna, J.-Y. Hogrel, P. G. Carlier, J. Vissing and V. Straub, 'Quantitative Muscle MRI as an Assessment Tool for Monitoring Disease Progression in LGMD2I: A Multicentre Longitudinal Study', PLoS ONE, 8 (2013): e70993.
5. D. M. Escolar, E. K. Henricson, J. Mayhew, J. Florence, R. Leshner, K. M. Patel and P. R. Clemens, 'Clinical evaluator reliability for quantitative and manual muscle testing measures of strength in children', Muscle Nerve, 24 (2001): 787-93.
6. J. M. Morrow, C. D. J. Sinclair, A. Fischmann, M. M. Reilly, M. G. Hanna, T. A. Yousry and J. S. Thornton, 'Reproducibility, and age, body-weight and gender dependency of candidate skeletal muscle MRI outcome measures in healthy volunteers', European Radiology, 24 (2014): 1610-1620.
7. S. Ponrartana, K. E. Andrade, T. A. Wren, L. Ramos-Platt, H. H. Hu, S. Bluml and V. Gilsanz, 'Repeatability of chemical-shift-encoded water-fat MRI and diffusion-tensor imaging in lower extremity muscles in children', AJR Am J Roentgenol, 202 (2014): W567-73.
8. D. V. Cicchetti, 'Guidelines, Criteria, and Rules of Thumb for Evaluating Normed and Standardized Assessment Instruments in Psychology', Psychological Assessment, 6 (1994): 284-90.
9. T. Zaraiskaya, D. Kumbhare and M. D. Noseworthy, 'Diffusion tensor imaging in evaluation of human skeletal muscle injury', J Magn Reson Imaging, 24 (2006): 402-8.
10. I. Miljkovic, A. L. Kuipers, R. Cvejkus, C. H. Bunker, A. L. Patrick, C. L. Gordon and J. M. Zmuda, 'Myosteatosis increases with aging and is associated with incident diabetes in African ancestry men', Obesity (Silver Spring, Md.), 24 (2016): 476-482.
Figures
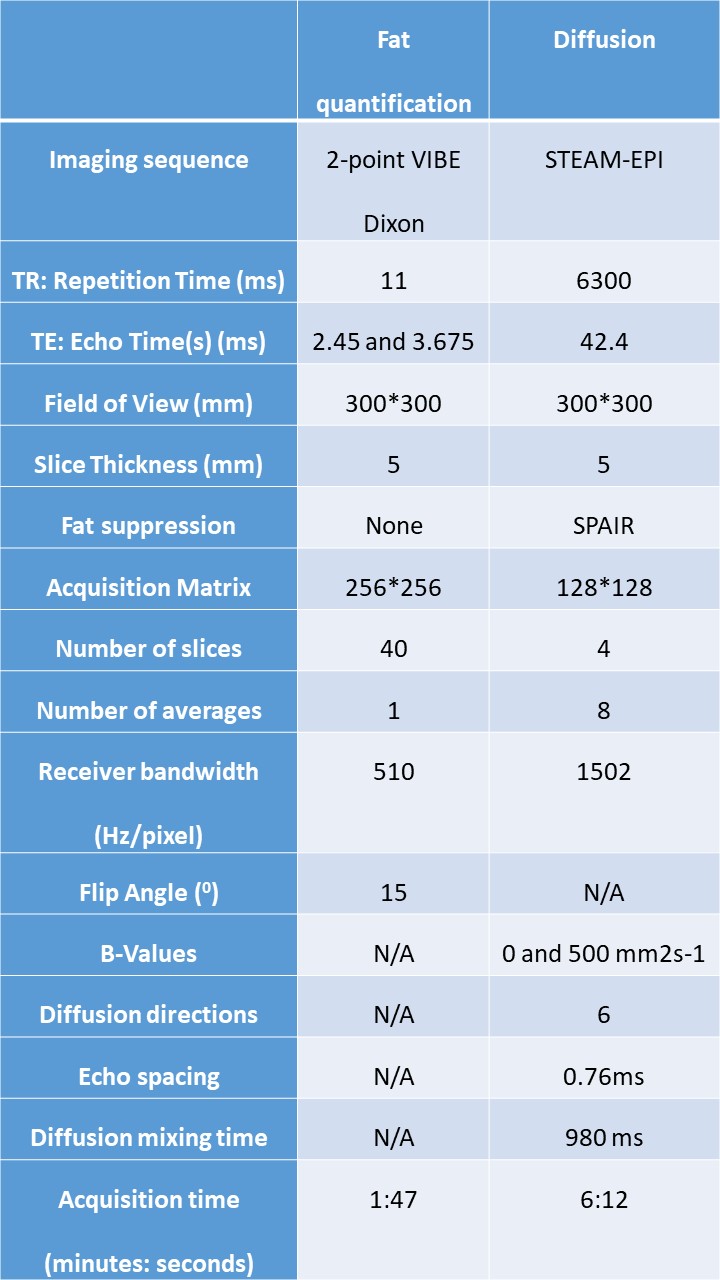
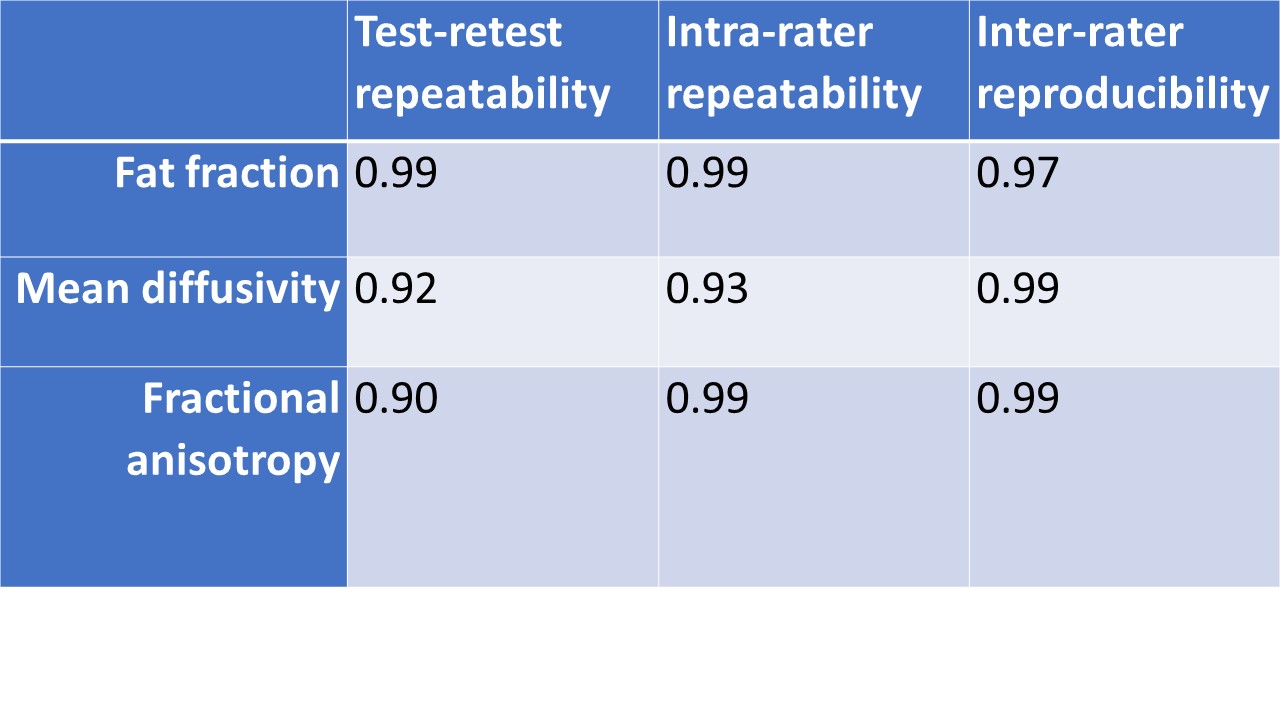
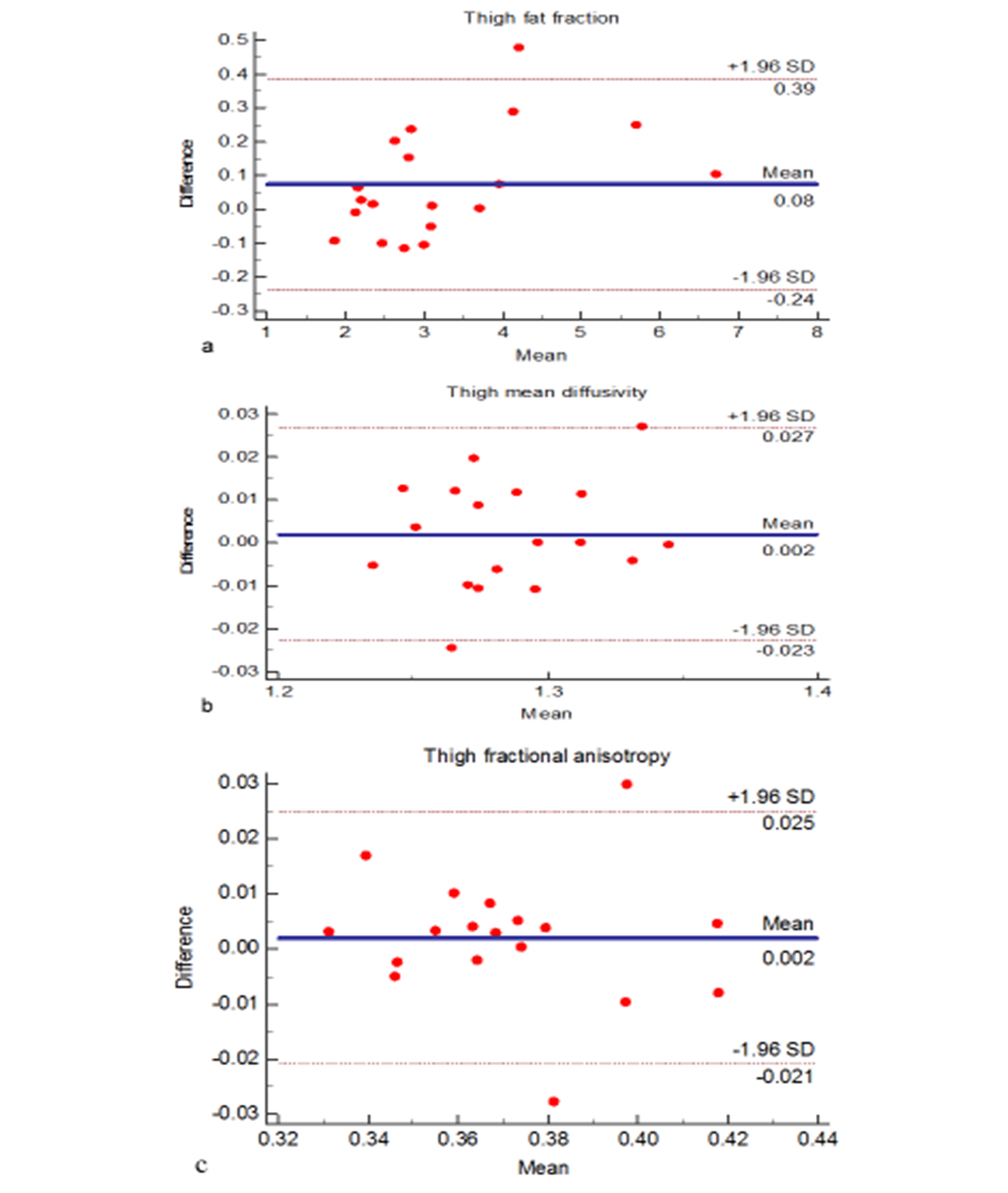
Figure 1: Test-retest repeatability
a) Fat fraction b) Mean diffusivity c) Fractional anisotropy
Figure 1 depicts the Bland-Altman plots showing the test-retest repeatability measurements with a 30-minute break in-between scans. The test-retest ICCs in the thigh were 0.99, 0.92 and 0.90 respectively.
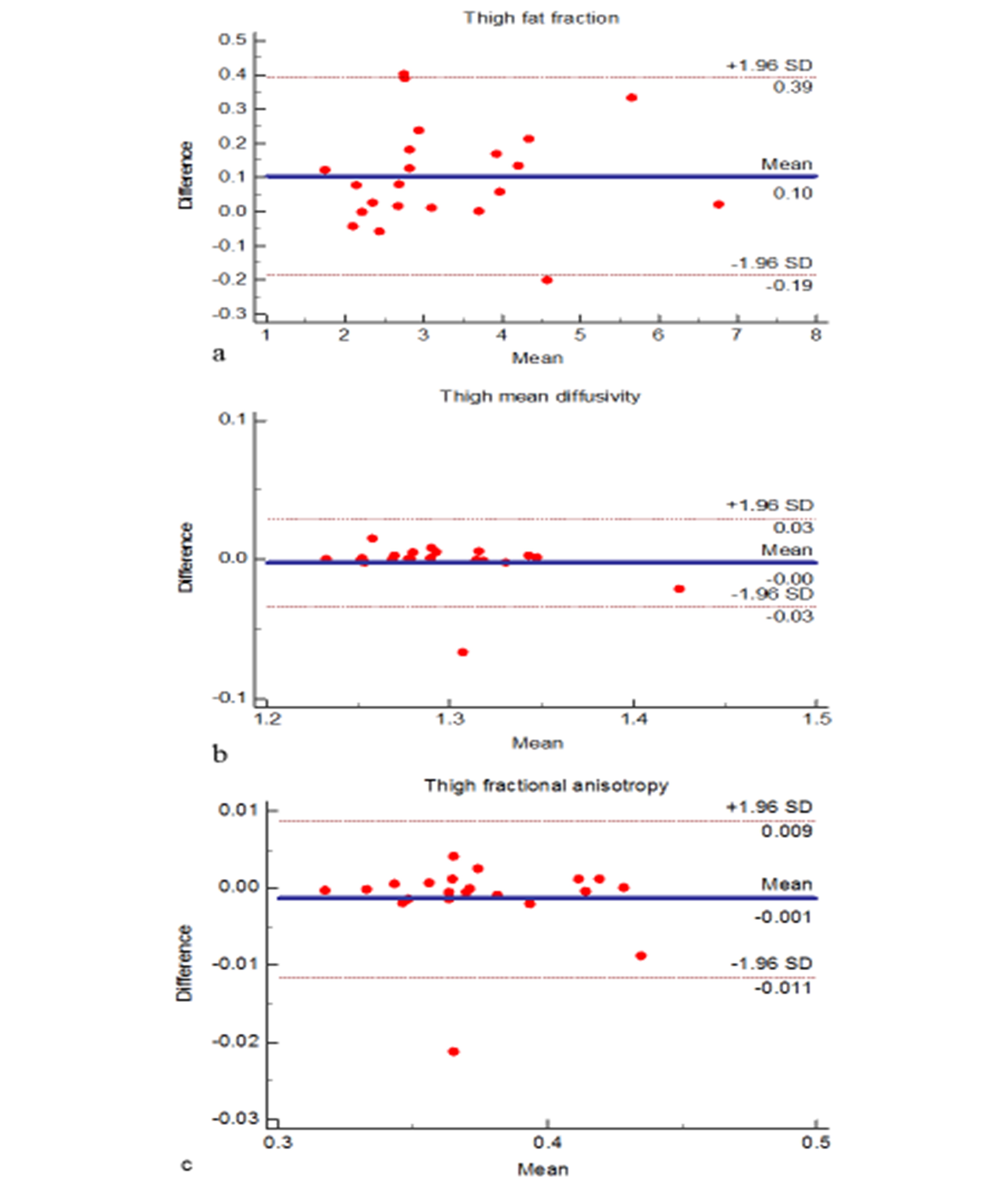
Figure 2: Intra-rater repeatability
a) Fat fraction b) Mean diffusivity c) Fractional anisotropy
Figure 2 depicts the Bland-Altman plots showing the intra-rater repeatability measurements. The intra-rater repeatability ICCs in the thigh were 0.99, 0.93, 0.99 respectively.
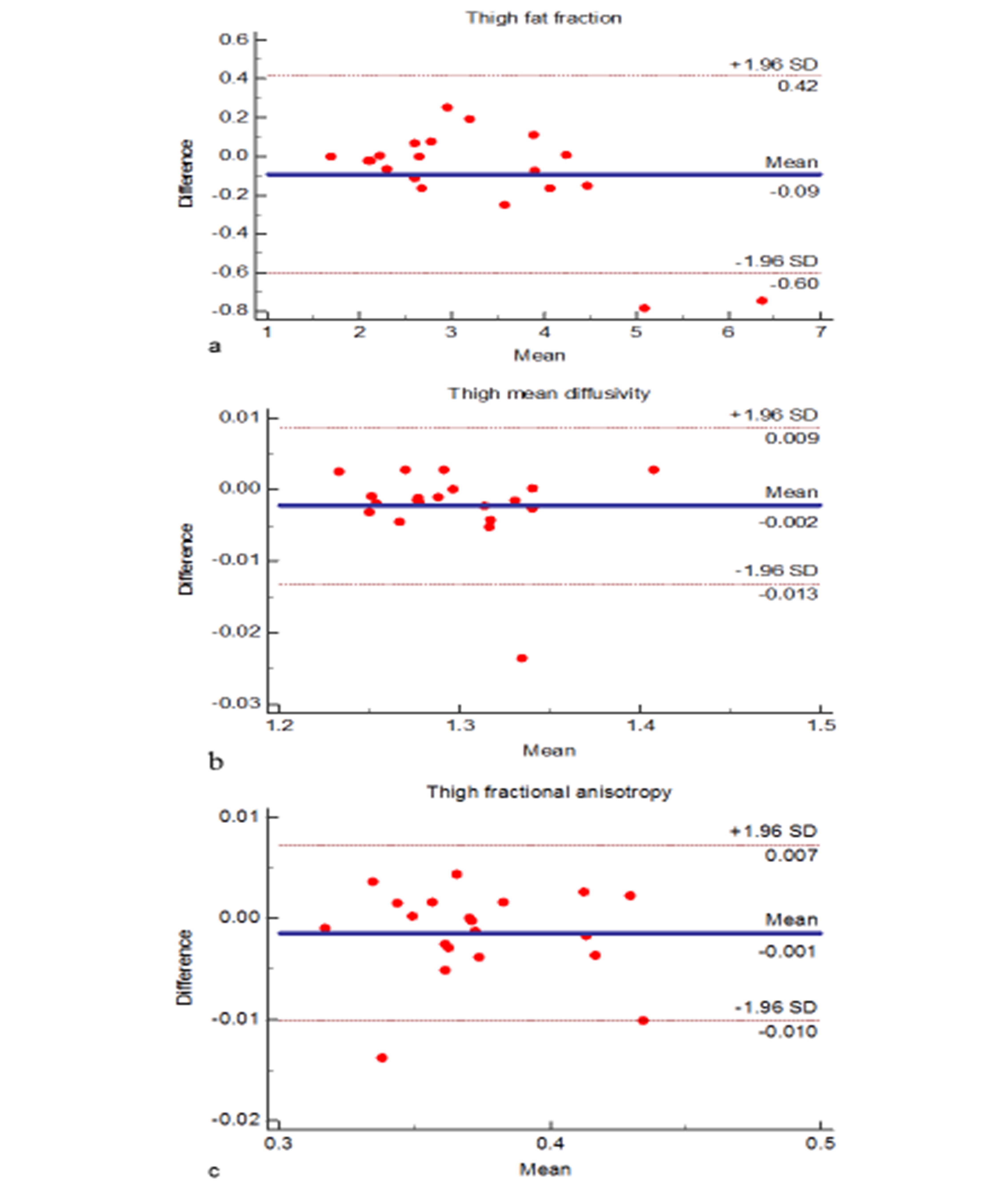
Figure 3: Inter-rater reproducibility
a) Fat fraction b) Mean diffusivity c) Fractional anisotropy
Figure 3 depicts the Bland-Altman plots showing the inter-rater reproducibility measurements. The intra-rater reproducibility ICCs in the thigh were 0.97, 0.99, 0.99 respectively.