5071
How reliable is DTI of the lower extremity muscles at high-field (3T) and ultra-high-field (7T) MRI?1High Field MR Center, Department of Biomedical Imaging and Image-Guided Therapy, Medical University of Vienna, Vienna, Austria, 2Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
The feasibility of DTI at 7T was already demonstrated for brain and muscles but, to date, the assessment of its reliability for calf muscles and a comparison with the reliability at 3T were still missing.Our results showed excellent ICCs(>.750) at 7T and 3T mainly for single muscles(e.g.,gastrocnemii’s tracks number).The comparison of absolute differences of the two consecutive measurements with each device demonstrated similar variability except for tracks’ number of the whole-calf(lower absolute difference at 7T;p=0.034) and FA of the gastrocnemius lateralis(lower absolute difference at 3T;p=0.032).Larger studies should further assess the overall performance of 7T for specific healthy and injured muscles.
Introduction
Diffusion Tensor Imaging (DTI) of skeletal muscle is affected by several challenges like, for instance, eddy-current-induced distortions due to high diffusion gradient amplitudes and poor signal-to-noise-ratio(SNR) due to the small T2/T1 ratio. Even if a stimulated echo acquisition mode sequence (STEAM) has demonstrated to improve DTI for muscle, ultra-high field can provide an additional advantage especially regarding SNR. Although the feasibility of DTI for brain and muscles at 7T has already been demonstrated [1,2], few studies evaluated the reliability of DTI for muscles at 3T [3,4] and, to the best of our knowledge, its assessment at 7T was still missing. Thus, we evaluated and compared the reliability of DTI measurements of calf muscles performed at high-field (3T) and ultra-high field (7T) MRI.Methods
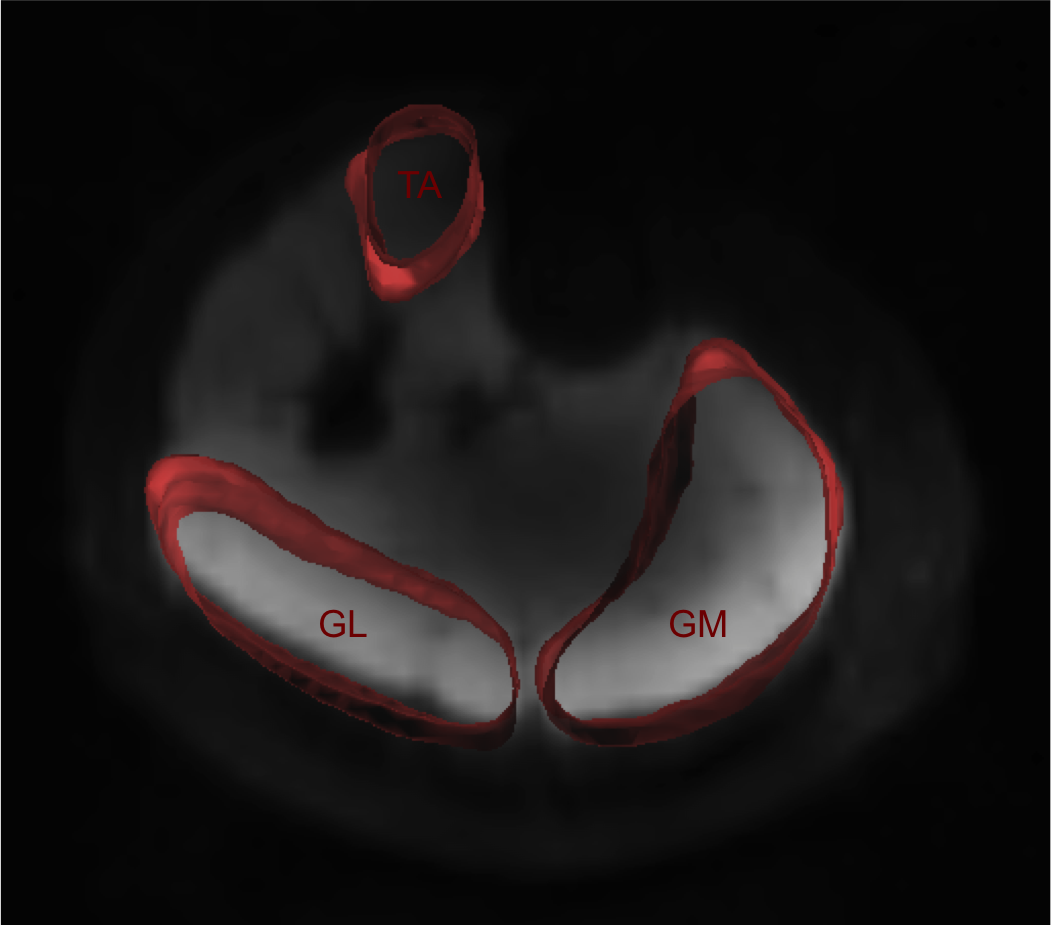
Ten volunteers (5 females; mean age 29.1±4.7years) without any history of muscle injuries/disease, were examined twice (i.e., during the same day and with complete repositioning) at 3T (MAGNETOM-Prisma, Siemens Healthcare, Erlangen, Germany) and 7T (Research Scanner, Siemens Healthcare, Erlangen, Germany), using a STEAM-DTI prototype sequence. SNR, DTI metrics (tracks’ number (tracksn), length (tracksl), volume (tracksv), fractional anisotropy (FA), mean (MD), axial (AD) and radial diffusivity (RD)) of the entire datasets (whole calf muscles, WCM), of tibialis anterior (TA), gastrocnemius medialis (GM) and lateralis (GL) were collected (Fig.1). Student’s T-tests were used to compare SNR and DTI metrics obtained at 3T and 7T. Intraclass-correlation coefficients (ICCs) were derived to assess the reliability of the consecutive DTI measurements at 3T and 7T [5]. Aiming to further assess the precision of the measurements obtained with each device, the absolute difference (i.e.,absolute difference between the two consecutive measurements with each device, for each volunteer, regarding WCM, TA, GM, and GL) was computed for each DTI metric at 3T and 7T and then compared (Student’s T-test).Results
The SNR was higher at 7T (+105.11%;p<.001). At 7T, tracksn, tracksv ,tracksl were higher for WCM, GM and GL (tracksn: +5.5%,+3.1%,+8.5%; tracksv: +12.1%,+12.2%,+14.7%; tracksl:+13.3%,+16.4%,+19.2%; p<.05,each) (Fig.2);TA showed only higher tracksn and tracksv (+6.3%,+16.4%; p<.05 each). MD and RD were higher at 7T for WCM (+1.3%, +1.8%; p<.05, each) and TA (+7.3%,8.9%; p<.05, each). TA showed higher FA at 3T(+3.1%; p=.001) and higher AD at 7T (+5.6%; p<.001). GM demonstrated lower MD and RD at 7T(-2.8%;-3.4%; p<.05). ICC was excellent (>.750) for both 7T and 3T regarding tracksn, tracksv and RD of GM and GL, RD of WCM and TA, and FA of WCM, GM and TA (Fig. 3).Excellent ICCs were obtained only at 3T for MD of GL and AD of WCM, GL and GM, and for FA of GL. No significant differences emerged comparing the absolute differences between the two consecutive measurements with each device, except for WCM’s tractsn (mean absolute difference at 7T=852;mean absolute difference at 3T=2273; p=0.034) and GL’s FA (mean absolute difference at 7T=0.019;mean absolute difference at 3T=0.007;p=0.032) (Fig. 4).Discussion
The results of our study, which is, to date, the first of its kind, investigating the reliability of DTI measurements of muscle not only at high but also at ultra-high field, has demonstrated that both 7T and 3T guarantee high reliability especially for single muscle analyses and regarding specific metrics.In the last decade, many studies focused on the optimization of DTI protocols for muscles, as well as on the feasibility of DTI evaluation of muscle anatomy, physiological changes and diseases but only few articles addressed the precision and reliability of DTI measurements in muscle imaging[3,4].Indeed, Froeling et al.[3],in agreement with our results, demonstrated a variation of the reliability according to the investigated area. Heemskerk et al. [4] showed that measurements performed during the same acquisition have a higher reliability than those performed within the same day or in different days. Even if in our study, both techniques showed excellent ICCs for specific metrics in some muscles, 3T showed an overall higher amount of metrics and muscles with higher reliability, these findings might be due to technical challenges associated with 7T imaging, like increased B0 and B1 inhomogeneity and chemical shift artifacts [6].Therefore the impact of these technical challenges on DTI metrics should be further addressed, aiming to take full advantage of the high SNR offered by ultra-high field imaging and improve the diagnostic performance of DTI for muscles at 7T.Conclusion
Despite the numerous challenges associated with DTI for muscles, both 3T and 7T demonstrated an excellent reliability mainly regarding single muscles.Future studies including a larger cohort are expected to further evaluate the overall performance of 7T for specific healthy and injured muscles.Acknowledgements
No acknowledgement found.References
1. Polders DL, Leemans A, Hendrikse J, et al. Signal to Noise Ratio and Uncertainty in Diffusion Tensor Imaging at 1.5, 3.0, and 7.0 Tesla. J Magn Reson Imaging. 2011 Jun;33(6):1456-63.
2. Giraudo C, Motyka S, Resinger C, et al. Diffusion Tensor Imaging of human muscle at ultra-high-field (7T) MR. ISMRM 25th Annual Meeting, 2017, Honolulu, HI, USA.
3. Froeling M, Oudeman J, van den Berg S, et al. Reproducibility of Diffusion Tensor Imaging in Human Forearm Muscles at 3.0 T in a Clinical Setting. Magn Reson Med. 2010;64(4):1182-90.
4. Heemskerk AM, Sinha TK, Wilson KJ, et al. Repeatability of DTI-based skeletal muscle fiber tracking. NMR Biomed. 2010;23(3):294-303.
5. Cicchetti DV. Guidelines, Criteria, and Rules of Thumb for Evaluating Normed and Standardized Assessment Instruments in Psychology. Pschological Assessment. 1994;6:284-290.
6. Umutlu L, Ladd ME, Forsting M, et al. 7 Tesla MR imaging: opportunities and challenges. Fortschr Röntgenstr 2014; 186:121-129.
Figures