4938
Effects of Track Length on White Matter Alterations in Mild Traumatic Brain Injury1Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, IN, United States, 2Department of Epidemiology and Biostatistics, Indiana University, School of Public Health, Bloomington, IN, United States, 3College of Engineering, Purdue University, West Lafayette, IN, United States, 4Department of Psychiatry, Dartmouth-Hitchcock Medical Center and Geisel School of Medicine, Hanover, NH, United States, 5Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, United States
Synopsis
In the present study, we performed streamline tractography to characterize effects of track length on white-matter microstructural alterations after mild traumatic brain injury. Streamline length and counts were studied in involved white-matter fiber tracts that were found to have decreased axonal density at some points along the tracts using voxel-based analyses. The results suggested that long fibers in the brains of individuals who sustained mild traumatic brain injury are more vulnerable to the injury.
Purpose
Mild traumatic brain injury (mTBI) is an important public health problem.1 Microscopically, diffuse axonal injury is generally believed to be the initial neuropathology associated with mTBI and leads to morphological changes of axons and the surrounding microenvironment.2-4 Therefore, diffusion MRI is recommended due to its sensitivity to microstructural changes in the brain white matter.5, 6 While ROI- and voxel-based analyses are used in more than 90% of published diffusion MRI studies on mTBI, tract-specific analyses have been less investigated. In voxel-based analyses, alterations of diffusion metrics in long-range fiber tracts (e.g., the corpus callosum, internal capsule, and longitudinal fasciculus) are frequently reported.7-10 Characterizing the susceptibility of fiber tracts to brain injury with respect to tract length, however, has not been studied. In this work, we performed streamline tractography and extracted tract-specific features including streamline counts and streamline length. We investigated the effect of track length on white matter microstructural alterations shortly after mTBI and clinical correlations.Material and Methods
Participants and MRI: A total of 42 subjects including 19 mTBI and 23 trauma-controls were recruited from the Emergency Department within 1 month post injury. The subjects underwent T1-weighted imaging with a MPRAGE sequence and multi-shell hybrid diffusion imaging (HYDI)11 in a Philips 3T Achieve TX scanner with SENSE parallel imaging. The diffusion encoding scheme consisted of 1 b0 and 5 b-value shells (b-values = 250, 1000, 2250, 4000, and 6250 s/mm2) with a total of 142 diffusion-weighting directions. Other imaging parameters are voxel size = 2x2 mm2, 40 slices of 3 mm slice thickness. Ten neuropsychological tests were performed to assess attention, memory, and executive function. The HYDI data were denoised with a LPCA method12 and corrected for motion, eddy current, and geometric distortion using the FSL eddy_openmp command.13 The preprocessed diffusion data were then fitted to neurite orientation dispersion and density imaging (NODDI)14 to extract intra-axonal volume fraction (Vic) inferring axonal density. Tractography: White-mater streamline tractography was performed using CAMINO15 software with a q-ball and spherical harmonic reconstruction for fiber orientation distribution functions. To extract cortical-to-cortical connections, white matter and gray matter interface was used as starting and destination points for tractography with a step size of 0.5 and iterations of 25. Involved white matter tracts were filtered by waypoint voxels that had significantly lower axonal-density (Vic) detected by track-based spatial statistics (TBSS) analyses (Figure 1A & B). Data Analysis: The tract-specific features (i.e., length and normalized streamline count) were summarized from the involved tracts and the rest uninvolved tracts (i.e., without waypoint filtering) for each mTBI and control subject. Paired t-tests, independent t-tests, and linear regression analyses were used for comparisons within subjects, between groups, and for correlations with neuropsychological outcomes, respectively.Results and Discussions
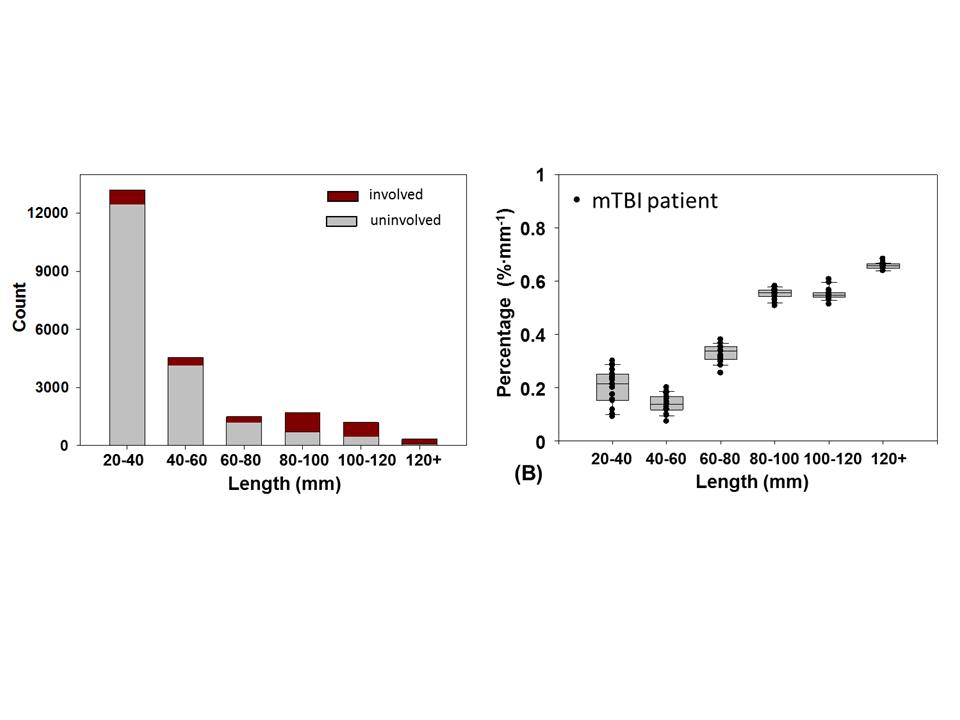
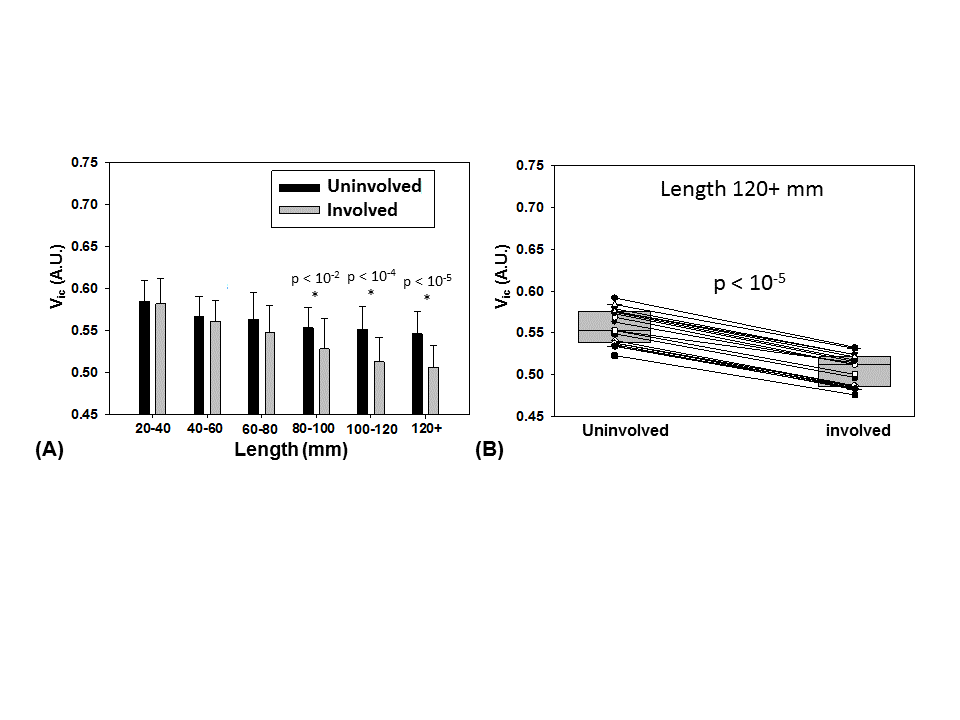
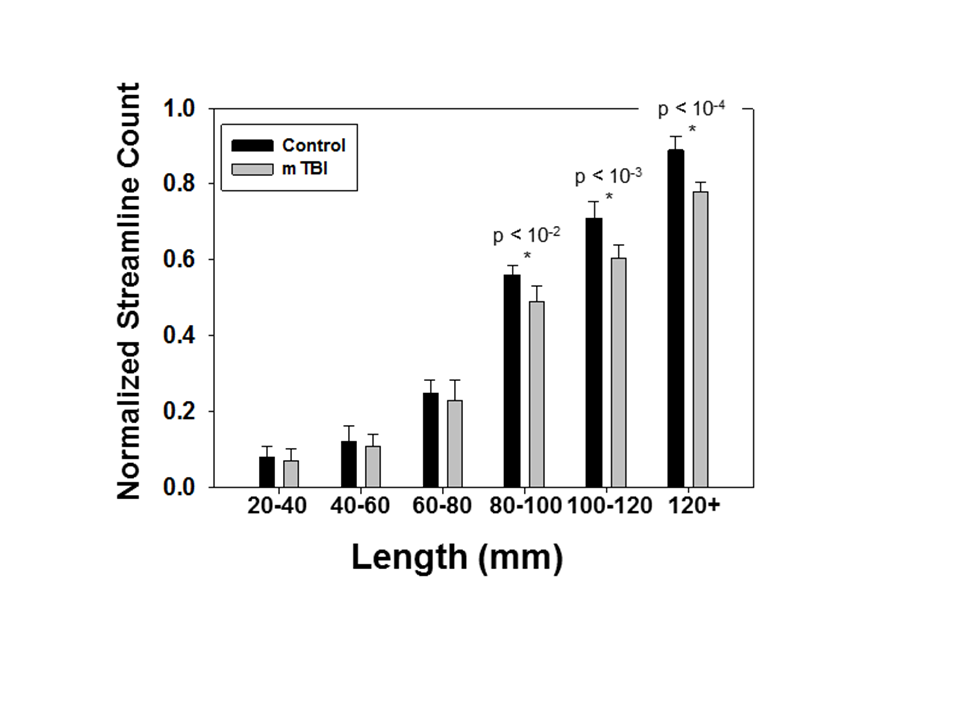
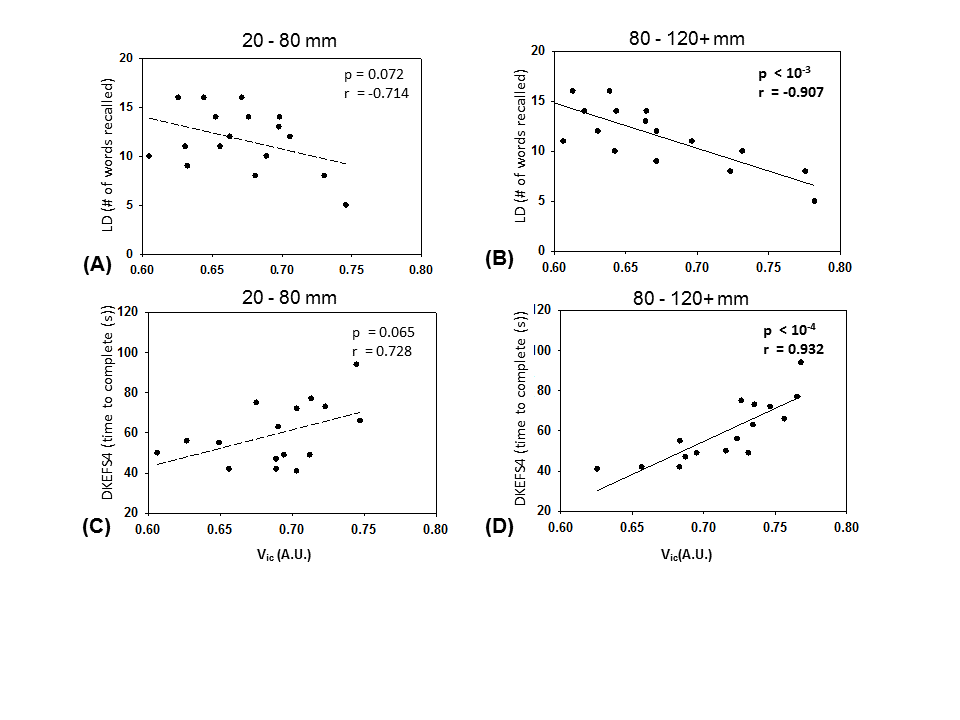
Three involved fiber tracts were identified: the forceps minor, superior corona radiata, and corticospinal tracts (Figure 1C). Figure 2A shows the prevalence of involved streamlines according to length. Figure 2B demonstrates that among the whole-brain streamlines, longer-length tracts had higher chance to have decreased axonal density at some points along the tracts after mTBI. To correct for inherent bias from tract length, the “chance" was defined as length-adjusted percentage (i.e., percentage of involved streamlines for that length category divided by streamline length). For a tract length longer than 80 mm, the length-adjusted percentage was between 0.6% and 0.7% per mm. In addition, in the involved tracts, longer streamlines had lower axonal density (Vic) throughout the tracts compared to the same length of streamlines in uninvolved tracts for each mTBI patient (Figure 3). The decrease in Vic in involved streamlines started to show significance at a length of 80-100 mm (Figure 3A), and reached p-value < 10-5 for streamlines longer than 120 mm (Figure 3B). Similarly, the mTBI patients had lower normalized streamline counts of longer tracts (Figure 4). The decrease in the streamline counts were significant at a length of 80 mm and higher. The averaged axonal density (Vic) throughout the involved tracts with a length longer than 80 mm correlated with neuropsychological measures for memory and executive function (Figure 5). The mTBI patients with higher Vic consistently had poor neuropsychological performance with fewer words recalled in memory function and longer time required to complete tests for executive function.Conclusion
In this study, we characterized the susceptibility of white-matter fiber tracts to the brain injury with respect to tract length. The white-matter fiber tracts longer than 80 mm appeared to be more vulnerable to the brain injury with lower axonal density, streamline counts, and significant clinical correlations.Acknowledgements
This study was supported by NIH R21 NS075791, NCAA-DoD Grand Alliance W81XWH-14-2-0151, and a Project Development Team within the ICTSI NIH/NCRR Grant Number UL1TR001108.References
1. Daneshvar, D.H., Nowinski, C.J., McKee, A.C., and Cantu, R.C. (2011). The epidemiology of sport-related concussion. Clin Sports Med 30, 1-17, vii.
2. Buki, A., and Povlishock, J.T. (2006). All roads lead to disconnection?--traumatic axonal injury revisited. Acta Neurochir (Wien) 148, 181-193; discussion 193-184.
3. Dikranian, K., Cohen, R., Mac Donald, C., Pan, Y., Brakefield, D., Bayly, P., and Parsadanian, A. (2008). Mild traumatic brain injury to the infant mouse causes robust white matter axonal degeneration which precedes apoptotic death of cortical and thalamic neurons. Exp Neurol 211, 551-560.
4. Spain, A., Daumas, S., Lifshitz, J., Rhodes, J., Andrews, P.J., Horsburgh, K., and Fowler, J.H. (2010). Mild fluid percussion injury in mice produces evolving selective axonal pathology and cognitive deficits relevant to human brain injury. J Neurotrauma 27, 1429-1438.
5. McCrea, M., Meier, T., Huber, D., Ptito, A., Bigler, E., Debert, C.T., Manley, G., Menon, D., Chen, J.K., Wall, R., Schneider, K.J., and McAllister, T. (2017). Role of advanced neuroimaging, fluid biomarkers and genetic testing in the assessment of sport-related concussion: A systematic review. Br J Sports Med 51, 919-929.
6. Wintermark, M., Sanelli, P.C., Anzai, Y., Tsiouris, A.J., Whitlow, C.T., and American College of Radiology Head Injury, I. (2015). Imaging evidence and recommendations for traumatic brain injury: Advanced neuro- and neurovascular imaging techniques. AJNR Am J Neuroradiol 36, E1-E11.
7. Hulkower, M.B., Poliak, D.B., Rosenbaum, S.B., Zimmerman, M.E., and Lipton, M.L. (2013). A decade of dti in traumatic brain injury: 10 years and 100 articles later. AJNR Am J Neuroradiol 34, 2064-2074.
8. Eierud, C., Craddock, R.C., Fletcher, S., Aulakh, M., King-Casas, B., Kuehl, D., and LaConte, S.M. (2014). Neuroimaging after mild traumatic brain injury: Review and meta-analysis. Neuroimage Clin 4, 283-294.
9. Gardner, A., Kay-Lambkin, F., Stanwell, P., Donnelly, J., Williams, W.H., Hiles, A., Schofield, P., Levi, C., and Jones, D.K. (2012). A systematic review of diffusion tensor imaging findings in sports-related concussion. J Neurotrauma 29, 2521-2538.
10. Dodd, A.B., Epstein, K., Ling, J.M., and Mayer, A.R. (2014). Diffusion tensor imaging findings in semi-acute mild traumatic brain injury. J Neurotrauma 31, 1235-1248.
11. Wu, Y.C., and Alexander, A.L. (2007). Hybrid diffusion imaging. Neuroimage 36, 617-629.
12. Manjon, J.V., Coupe, P., Concha, L., Buades, A., Collins, D.L., and Robles, M. (2013). Diffusion weighted image denoising using overcomplete local pca. PLoS One 8, e73021.
13. Andersson, J.L., and Sotiropoulos, S.N. (2016). An integrated approach to correction for off-resonance effects and subject movement in diffusion mr imaging. Neuroimage 125, 1063-1078.
14. Zhang, H., Schneider, T., Wheeler-Kingshott, C.A., and Alexander, D.C. (2012). Noddi: Practical in vivo neurite orientation dispersion and density imaging of the human brain. Neuroimage 61, 1000-1016.
15. Cook, P.B., Y; Nedjati-Gilani, S; Seunarine, KK; Hall, MG; Parker, GJ; Alexander, DC. Camino: Open-source diffusion-mri reconstruction and processing. in ISMRM. 2006. Seattle, WA, USA.
Figures