4933
Quantifying brain oxygen extraction fraction: correlation between a global venous susceptibility method and calibrated fMRI mapping method.1CUBRIC, School of Psychology, Cardiff University, Cardiff, United Kingdom, 2Nuffield Department of Clinical Neurosciences, Oxford University, Oxford, United Kingdom, 3Department of Radiology, University of Pennsylvania, Philadelphia, PA, United States, 4School of Medicine, Cardiff University, Cardiff, United Kingdom, 5Siemens Healthcare Ltd, Camberley, United Kingdom, 6School of Physics and Astronomy, Cardiff University Brain Research Imaging Centre, Cardiff University, Cardiff, United Kingdom
Synopsis
Measuring oxygen extraction fraction (OEF) may prove a useful clinical tool for assessing brain oxygen consumption. Dual-calibrated fMRI is used to map voxel-wise OEF across grey-matter and requires respiratory challenge (hypercapnia and hyperoxia). However, this method presents challenges to clinical implementation. Conversely, OxFlow provides a global estimate of OEF, has a shorter acquisition time and does not require respiratory challenge. Here we examine the relationship between both approaches for measuring OEF, revealing a significant association between methods. While further investigation is required, OxFlow may offer additional clinical utility for measuring cerebral oxygen consumption.
Introduction/Purpose
Measuring oxygen extraction fraction (OEF) with MRI may prove a useful clinical tool for assessing brain oxygen consumption and tissue energetics. Several MRI methods have recently been developed to quantify OEF, including dual-calibrated fMRI and OxFlow. Dual-calibration fMRI has been developed to map grey matter OEF at the voxel-wise level requiring respiratory challenge (hypercapnia and hyperoxia).1,2 However, this method relies on physiological assumptions and presents challenges to implementation in clinical practice. Conversely, global estimates of OEF using methods such as OxFlow are quicker to acquire, do not require respiratory challenge and rely on fewer assumptions.3,4 Here, we directly compare OEF estimates between OxFlow (sagittal sinus susceptibility) and our dual-calibrated fMRI method of measuring brain oxygen consumption.Methods
The current study employed two approaches to estimate OEF. First, we used an home built dual-excitation PCASL based dual-calibration method to map changes in oxygen metabolism and OEF across grey matter, by acquiring CBF and BOLD signals together.1,2 Scan parameters - TE1: 10ms, TR1: 3600ms, TE2: 30ms, TR2: 800ms, slice thickness: 7mm, and GRAPPA acceleration factor 3. Acquisition time for the PCASL sequence was 18 minutes, during which hypercapnic and hyperoxic respiratory stimuli were presented. Second, we used the OxFlow sequence that calculates SvO2 in the superior sagittal sinus through susceptometry-based oximetry 3,4. Acquisition time for the OxFlow sequence was 1.17 minutes. Imaging parameters: TR=35ms, ∆TE=7.04ms, SSS level FOV=208×208mm2/ voxel size=1×1×5mm3, neck level FOV=176×176mm2/voxel size=0.85×0.85×5mm3, FA=15° and scan duration 1.17 minutes. In addition, we acquired a TOF head (for localizing the SSS in the OxFlow sequence), a phase-contrast flow scan for localizing neck vessels (for both OxFlow and ASL sequences) and a T1-MPRAGE for brain volume estimation. Measurements were performed on a clinical 3T scanner (Prisma MAGNETOM, Siemens Healthcare, Erlangen, Germany). In a mixed group of 15 individuals (7 with repeated measurements) we assessed the consistency between the two methods for calculating grey matter/whole brain OEF. The group of participants originate from two separate studies. This includes a group of healthy individuals (n=11), some of which were scanned twice (n=7), and patients with multiple sclerosis scanned once (n=4). Analysis included linear mixed modelling to look at the association between both methods for calculating OEF. This approach helped to maximize power while controlling for repeated measures aspects of the study.Results
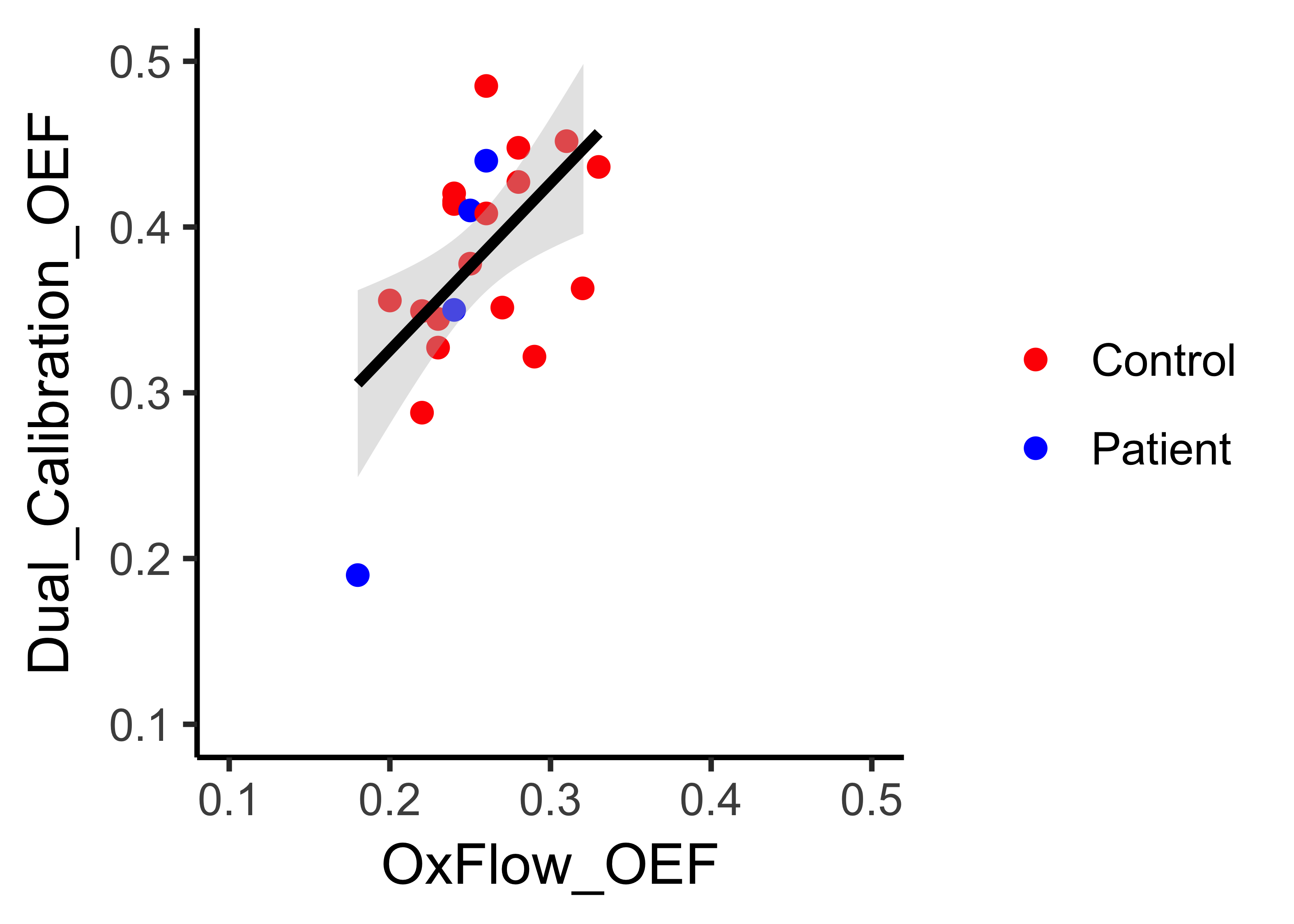
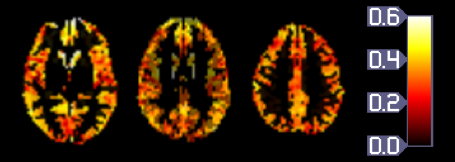
Results of the linear mixed modelling analysis revealed a significant positive relationship between OxFlow (mean=.25, SD=.04) and the dual-calibrated fMRI method (mean=.38, SD=.07) (β=.71, t=2.79, p=.033, adjusted for repeated-measures). These results suggest that there is a significant association between both methods in estimating OEF. A graphical representation of this relationship can be observed in Figure1.In addition, Figure2 represents an individual subjects grey matter OEF map from the dual-calibration fMRI method.Discussion and Conclusions
We establish a positive relationship between OEF measures derived from the dual-calibration fMRI and OxFlow methods. While dual-calibration is able to detect regional changes in OEF 5, OxFlow provides a comparable global estimate of OEF in a shorter session, without need for respiratory challenges. While there is a significant agreement between the methods, the dual-calibrated mapping method appears to give higher estimations of OEF and there is considerable scatter around the best-fit line. Bias is possible in both methods, for example, arising from violation of assumptions of isometabolism during hypercapnia and hyperoxia or non-ideal geometry of the sagittal sinus. In addition, dual-calibrated mapping method is only able to measure OEF in grey matter, while OxFlow assesses OEF across grey and white matter. The sources of disagreement between the methods require further investigation. However, the OxFlow method of measuring OEF may offer additional clinical utility and feasibility, where OEF mapping, provided by dual-calibration approaches, is not required.Acknowledgements
We would like to acknowledge support from the Wellcome Trust [WT200804], UK Engineering and physical sciences research council [EP/K020404/1], The Waterloo Foundation and Neuroscience and Mental Health Research Institute.References
1Germuska, M., Merola, A., Murphy, K., Babic, A., Richmond, L., Khot, S., Hall, J.E. and Wise, R.G., 2016. A forward modelling approach for the estimation of oxygen extraction fraction by calibrated fMRI. NeuroImage, 139, pp.313-323.
2Schmithorst, V.J., Hernandez-Garcia, L., Vannest, J., Rajagopal, A., Lee, G., Holland, S.K., 2014. Optimized simultaneous ASL and BOLD functional imaging of the whole brain. J Magn Reson Imaging 39, 1104-1117.
3Jain, V., Langham, M.C. and Wehrli, F.W., 2010. MRI estimation of global brain oxygen consumption rate. Journal of Cerebral Blood Flow & Metabolism, 30(9), pp.1598-1607.
4Barhoum, S., Langham, M. C., Magland, J. F., Rodgers, Z. B., Li, C., Rajapakse, C. S., & Wehrli, F. W. (2015). Method for rapid MRI quantification of global cerebral metabolic rate of oxygen. Journal of Cerebral Blood Flow & Metabolism, 35(10), 1616-1622.
5Merola, A., Murphy, K., Stone, A.J., Germuska, M.A., Griffeth, V.E., Blockley, N.P., Buxton, R.B. and Wise, R.G., 2016. Measurement of oxygen extraction fraction (OEF): An optimized BOLD signal model for use with hypercapnic and hyperoxic calibration. NeuroImage, 129, pp.159-174.
Figures