4908
Reduced Specific Energy Deposition with Diagnostic Image Quality in Pediatric Population using CArdioREspiratory Synchronized (CARESync) Balanced Steady-State Free Precession Cine Imaging1Radiology, Texas Children's Hospital, Houston, TX, United States, 2Cardiology, Texas Children's Hospital, Houston, TX, United States
Synopsis
Cine-bSSFP cardiac imaging in sedated pediatric population faces two-fold challenges: 1) respiratory motion; and 2) cardiocirculatory impairment associated compromised thermoregulatory response. Prospective 63 sedated patients’ study shows that CAdioREspiratory Synchronized sequence, with prospective arrhythmia rejection and retrospective cardiac gating, reduced specific absorbed energy per slice in fixed (18.96±5.16 J/kg) by 49.36% and adaptive (24.13±9.55 J/kg) by 39.24% modes, than equivalent 4NSA sequence while maintaining spatial, temporal, and contrast resolutions possible with breath-holds, providing consistently good image quality with 21.13% increased scan time (26.38±8.15 s) per slice. Adaptive mode reduced scan time by 18% than fixed mode for favorable cardiorespiratory rates.
Puspose
To prospectively evaluate the image quality and specific absorbed energy of fixed mode and adaptive mode CArdio-REspiratory Synchronized (CARESync) balanced steady-state free precession (bSSFP) sequence for acquiring cardiac cine images during free breathing in sedated and un-sedated pediatric patients with prospective arrhythmia rejection and retrospective cardiac getting and diagnostic spatial and temporal resolutions.Background
Cardiac cine balanced steady-state free precession (bSSFP) imaging faces two-fold challenges in pediatric patients: 1) bulk motion artifacts as patients below 7 years of age have to be sedated or many other are unable to suspend respiration consistently for sufficient time; and 2) thermoregulatory response in these patients is compromised due to impaired cardiovascular function and they cannot communicate heating issues due to sedation. While it is necessary to acquire cine bSSFP images in free breathing, it is important to maintain features like prospective arrhythmia rejection and retrospective gating to acquire complete cardiac cycle and also be prudent to ensure that overall specific absorbed energy (SAE) does not exceed 1.8 kJ/kg (0.5°C rise in body temperature) in sedated pediatric patients with cardiovascular disease [1]. Traditional approach to obviate the need for breathholding via respiratory gating (RG) or multiple number of signal averages (mNSA) impose a significant RF energy deposition for bSSFP cine imaging, due to the uninterrupted application of high-flip angle RF pulses throughout the acquisition. A CARESync approach with interruptions in RF deposition could mitigate these challenges by reducing the effective specific absorption rate (SAR) and the total SAE.Methods
All imaging for this IRB approved prospective study was performed on a 1.5T clinical MR scanner (Ingenia, Philips Healthcare) in 63 sedated patients (age 11.7±10.3, range 4mo-58yrs; 40 male; HR 85.2±18.1, range 48-140hbm; Resp 20.8±5.9, range 12-38 rpm). MRI: CARESync sequence described in Fig1 allows two free breathing modes: fixed – single R-R per respiration, and adaptive – multiple R-R per respiration with prospective rejection for inspiration during acquisition. The imaging parameters were: TR/TE/FA=2.5-2.7ms/1.25-1.35ms/60°; acquired voxel size: 1.65-2x1.65-2x5-8 mm3; SENSE=1.3-2; temporal resolution 30-45ms. Data Analysis: Experienced CMR reader, blinded to CARESync mode, graded image quality (IQ) for all sedated CMR scans (June-Sept 2017), based on: blood to myocardial contrast, signal uniformity, and delineation of the endocardial contour throughout the cardiac cycle, on the scale of 1 to 5 where 5 corresponds to IQ equivalent to best possible with breath-hold sequence (Fig2). Actual acquisition times, RF transmission, and physiology events were retrieved from scanner log files. Equivalent four number of signal averages (4NSA) scan times, RF duty cycle, effective SAR and SAE were calculated using logged data. Paired and two-sample t-tests were performed to compare RF dose and acquisition times.Results
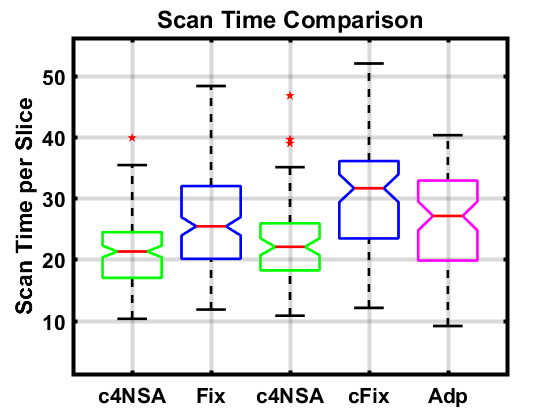
All 63 sedated patients were scanned without any issues with CARESync by two CMR experienced technologist without any supervision (41 fixed mode). IQ scores ranked as excellent (26.5%), good (66%), to moderate (7.5%) from 253 sequences (63 SA, 63 VLA, 53 4CH, 25 LVOT, 30 RVOT, 19 AoRoot) (Fig3). The IQ scores for fixed and adaptive mode (p=0.40 two-sided Wilcoxon signed ranked test) were comparable. SAE per slice was reduced in fixed mode (18.96±5.16 J/kg) by 49.36% and in adaptive mode (24.13±9.55 J/kg) by 39.24% compared to equivalent computed 4 NSA from logged R-Rs (c4NSA) sequence (Fig4). The mean rate of energy deposition for the CARESync sequence was lower than c4NSA (1.76±0.09 kJ/kg/min) sequence by 46.4% in fixed mode (0.93±0.17 kJ/kg/min) and 58.6% % in adaptive mode (0.73±0.12 kJ/kg/min) (Fig 4). The acquisition duration per slice for adaptive mode (26.1±8.8s) was significantly shorter (18%, p<0.0017) than for the fixed mode computed from logged cardiorespiratory rates (31.8±12.2s) (Fig5). The acquisition duration per slice for CARESync (26.28±8.15s) was significantly longer (p<0.0001) than c4NSA (21.8±6.2s). Fixed mode of CARESync has been previously reported to improve IQ significantly over multi-NSA and provide comparable ventricular volumes [2].Conclusion
Cardio-respiratory synchronized (CARESync), retrospectively cardiac–gated bSSFP sequence with prospective arrhythmia rejection provides the ability to prescribe multi-slice, multi-phase bSSFP sequences with significantly lower SAE (50-60%) and SAR (45-55%) burden compared to alternative of respiratory gated or four signal averaging sequences. CARESync provides consistently good image quality equivalent of breath-hold acquisitions in sedated pediatric CMR studies. Adaptive mode allows further 18% reduction in scan time compared to fixed mode for favorable cardiorespiratory rates.Acknowledgements
No acknowledgement found.References
[1] The International Commission on Non-Ionizing Radiation Protection. MEDICAL MAGNETIC RESONANCE (MR) PROCEDURES: PROTECTION OF PATIENTS. Health Phys. 2004;87:197–216.
[2] Krishnamurthy R, Pednekar A, Atweh LA, Vogelius E, Chu ZD, Zhang W, et al. Clinical validation of free breathing respiratory triggered retrospectively cardiac gated cine balanced steady-state free precession cardiovascular magnetic resonance in sedated children. J Cardiovasc Magn Reson. 2015;17.
Figures