4900
One Minute Free Breathing 3D Cardiac Cine MRI Using Data Clustering for Respiratory Self-Gating with Subject-Adaptive Gating Efficiency1Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 2Global MR Applications and Workflow, GE Healthcare, Menlo Park, CA, United States, 3University of California San Francisco, San Francisco, CA, United States
Synopsis
Conventional 2D cine MRI for cardiac functional measurements requires a series of breath-holds, which is usually difficult for children or sick patients and often results in non-diagnostic images. We aim to develop a fast and reliable free-breathing 3D imaging technique, which also allows subject-specific respiratory motion compensation.
INTRODUCTION
3D cardiac cine MRI
techniques have been developed to overcome limitations of the current standard
breath-hold 2D cine imaging, either during a single breath-hold or free
breathing. The cardiac image quality heavily relies on the subject’s
breathholding capability or reliable compensation of respiratory motion during
free breathing imaging, both can vary substantially among subjects. In this
study, we tested a 3D cine imaging method which only requires one minute scan
time during free breathing and allows robust and reliable motion compensation by
using a data-adaptive scheme to determine respiratory self-gating efficiency
for individual subjects. MATERIALS AND METHODS
Accelerated free-breathing 3D
cardiac cine imaging has been developed using a pseudo-random variable-density undersampling
strategy, CIRcular Cartesian UnderSampling (CIRCUS) [1]. Similar to many other
self-gating methods, respiratory gating efficiency was manually chosen (such as
an empirical range between 25%-50% can generate reasonable motion compensation).
We aim to improve the motion compensation strategy while further reducing scan
time.
One minute free breathing 3D cine MRI was applied to
cover the left ventricle (LV) in a short axis view on 3 healthy volunteers at a
3.0T MR scanner (GE Medical Systems, Milwaukee, WI) with an 8-channel cardiac
coil. The imaging parameters were: FOV = 34.0×25.5 cm2, TR/TE =
3.5/1.4ms, flip angle = 45°, readout bandwidth = ± 125kHz, slice thickness = 8
mm, image matrix = 192×144, and number of slices = 16. Prospective ECG triggering
was applied. 20 cardiac phases were reconstructed using a combined compressed
sensing and parallel imaging reconstruction method (k-t SPARSE-SENSE method)
[2,3].
The variable-density k-space data acquisition using
CIRCUS repeatedly acquires a center k-space line along kx and the calculated cross-correlation of those center
lines can provide respiratory motion tracking [1], by exploiting their
principle correlation using principle component analysis (PCA). Here we applied
k-means clustering on the derived gating signal to four clusters, which can represent
the respiratory motion from end-expiration to end-inspiration (and the two
transition phases in between), and then the data corresponding to the cluster
with minimal average distance (minimal intra-cluster motion) was chosen for
image reconstruction.
Conventional 2D cine and
single breath-hold 3D cine MRI sequences were also acquired for comparison. The
2D cine MRI was acquired with a lower in-plane resolution (2.4×2.2mm). The
single breath-hold 3D cine had the same scan settings as the free breathing
sequence, but with a conventional segmented view ordering instead of CIRCUS
patterns.
The subject-adaptive self-gating scheme has also been
tested in 4D flow cardiac MRI, with scan parameters: FOV = 34.0×25.5 cm2,
TR/TE = 6.3/3.1ms, flip angle = 8°, readout bandwidth = ± 125kHz, slice
thickness = 8 mm, image matrix = 180×136, number of slices = 16, and scan time
of ~ 5 mins. RESULTS AND DISCUSSION
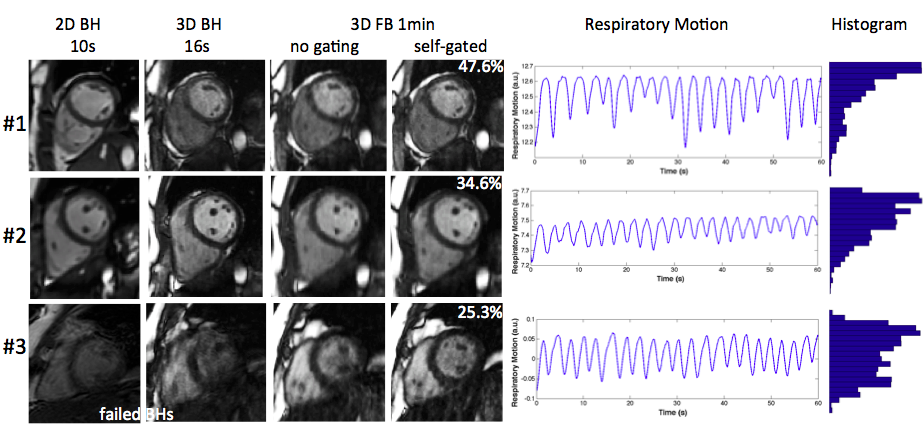
One
minute free breathing 3D cine MRI has been successfully applied on all three
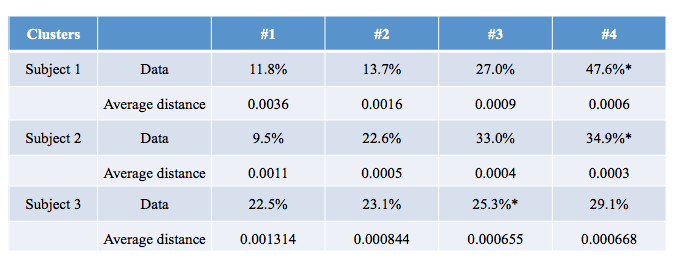
healthy subjects (shown in Figure 1). The subject-adaptive respiratory gating
efficiencies were calculated using k-means clustering (Table 1 shows the data
distribution for the clusters). Overall, free-breathing 3D cardiac cine images
with CIRCUS sampling strategy have inherent motion robustness due to use of
spiral-like sampling trajectory and oversampling at central k-space. For
respiratory pattern that contains a longer period of time at end-expiration
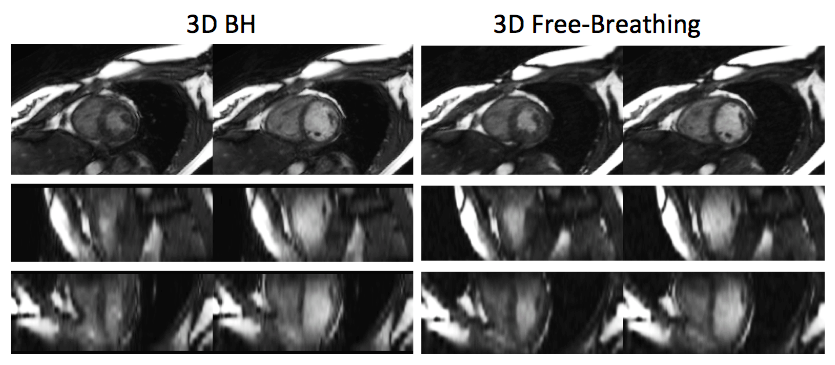
(case #1), the self-gated free-breathing method could provide almost identical image
quality to those acquired with the single breath-hold 3D MRI (first row in
Figure 1 and Figure 2). For the subject who barely could hold his/her breath
(case #3), both 2D and 3D breath-hold MRI suffer from severe motion artifacts,
however, the free-breathing method with the subject-adaptive respiratory gating
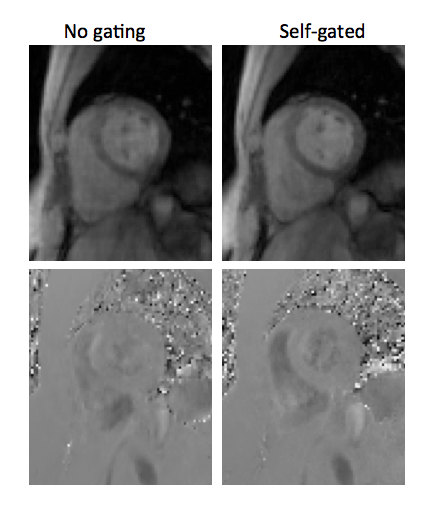
provides diagnosable image quality (third row in Figure 3). Figure 3 demonstrated
the improvements in the images of self-gated 4D flow cardiac MRI using the subject-adaptive
respiratory gating. CONCLUSIONS
We have developed a one-minute
free-breathing 3D cine MRI technique with subject-adaptive respiratory gating
efficiency, which provides reliable image quality regardless of the respiratory
motion pattern of the subject. Acknowledgements
NIH K25 EB014914 (JL), NIH R56HL133663 (JL), GE Healthcare Research Grant (JL).References
1. Liu J, Feng L, Shen HW, Zhu C, Wang Y, Mukai K, Brooks GC, Ordovas K, Saloner D. Highly-accelerated self-gated free-breathing 3D cardiac cine MRI: validation in assessment of left ventricular function. MAGMA. 2017 Aug; 30(4):337-346.
2. Otazo R, Kim D, Axel L, Sodickson DK. Combination of compressed sensing and parallel imaging for highly accelerated first-pass cardiac perfusion MRI. Magn Reson Med. 2010;64(3):767-76. Epub 2010/06/11. doi: 10.1002/mrm.22463. PubMed PMID: 20535813; PubMed Central PMCID: PMC2932824.
3. Feng L, Srichai MB, Lim RP, Harrison A, King W, Adluru G, Dibella EV, Sodickson DK, Otazo R, Kim D. Highly accelerated real-time cardiac cine MRI using k-t SPARSE-SENSE. Magn Reson Med. 2013;70(1):64-74. doi: 10.1002/mrm.24440. PubMed PMID: 22887290; PubMed Central PMCID: PMC3504620.
Figures