4899
Real life application of compressed sensing cardiac MRI for biventricular response to exercise.1Richard Slaughter Centre of Excellence in Cardiovascular MRI, The Prince Charles Hospital, Brisbane, Australia, 2Menzies Health Institute, Griffith University, Gold Coast, Australia, 3School of Allied Health Sciences and Menzies Health Institute, Griffith University, Gold Coast, Australia, 4Allied Health Research Collaborative, The Prince Charles Hospital, Brisbane, Australia, 5Physiotherapy Department, The Prince Charles Hospital, Brisbane, Australia, 6Siemens Healthineers, Sydney, Australia
Synopsis
Accurate assessment of left and right ventricular function using cardiac MRI plays an important role in the management of cardiac diseases. Combined with exercise stress testing, unveiling of cardiac diseases in the latent phase permits early initiation of appropriate therapy. Using compressed sensing cardiac MRI, we demonstrated dynamic quantitative biventricular functional assessment is safe and highly feasible for clinical utility.
Introduction
Cardiac magnetic resonance imaging (MRI) is the established reference standard for assessing biventricular volumes and systolic function at rest.1 Due to practical and technical limitations of imaging, clinical cardiac assessment is conventionally performed with the patient at rest. However, in many cardiac diseases, symptoms do not occur at rest and ventricular assessment during exercise is necessary to unmask ventricular dysfunction that is not apparent at rest. While MRI has superior temporal and spatial resolution and endocardial definition compared to standard techniques for stress imaging such as echocardiography and nuclear imaging, standard ECG-gated cine SSFP imaging is challenging during exercise. Ultra-fast acquisition is required to achieve full ventricular coverage while maintaining peak heart rate during a short breath-hold. We assessed the feasibility of a modified prototype balanced steady-state free precession cine sequence with compressed sensing (CS_bSSFP) under exercise conditions in clinical patients and controls.Method
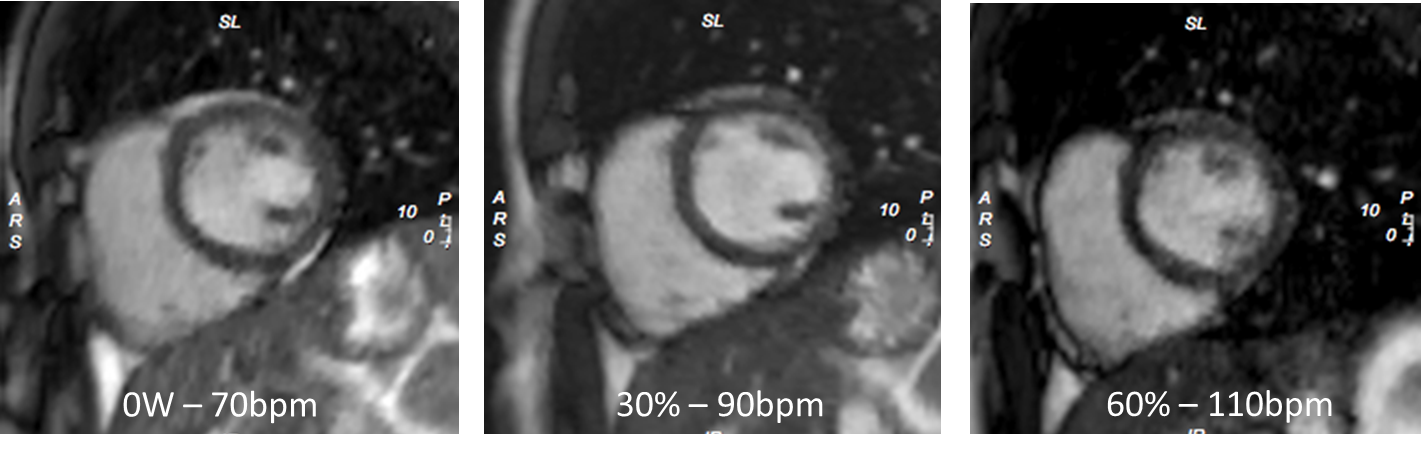
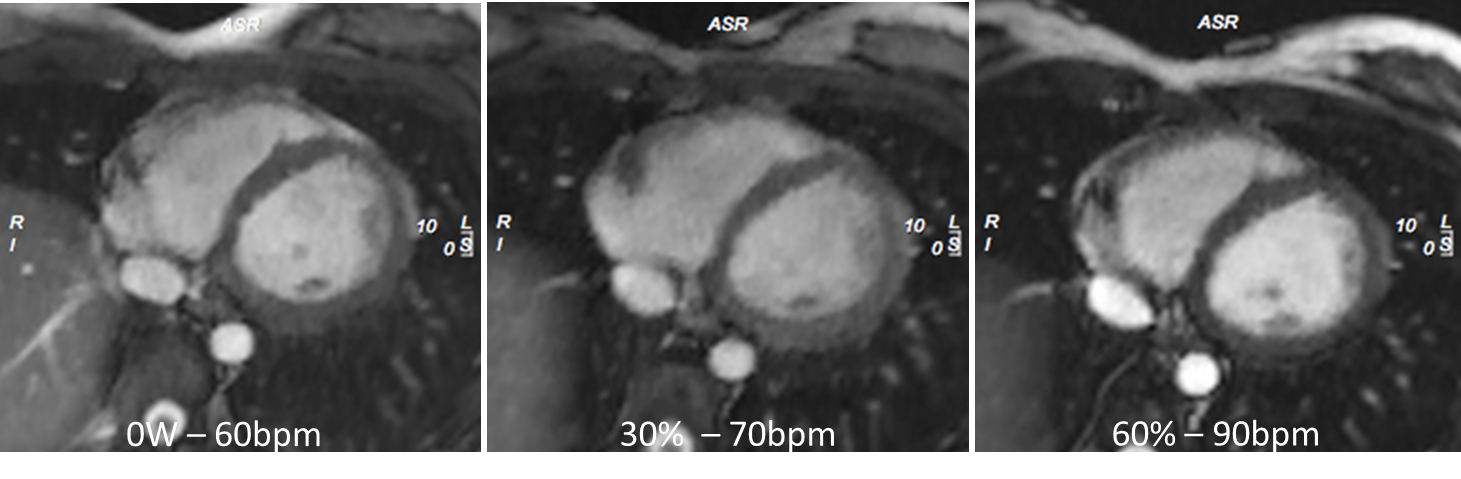
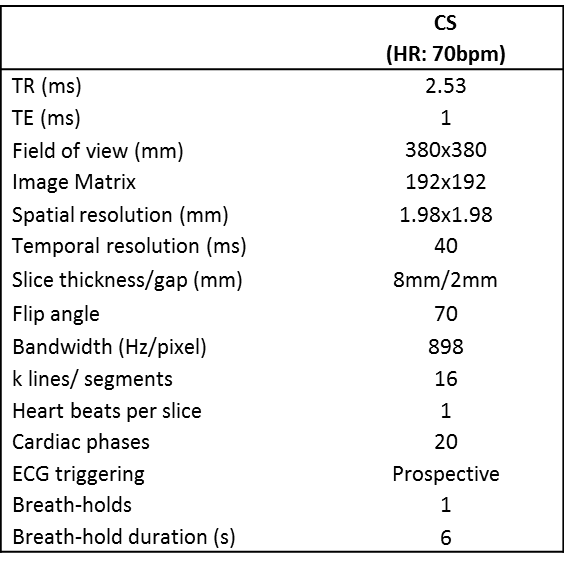
MRI was performed on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) using an 18-channel phased array cardiac coil. An electromagnetically braked MRI cycle ergometer (Lode, Groningen, Netherlands) was used for exercise ergometry prior to the MRI scan and for subsequent exercise MRI. MRI data were acquired with a prototype CS_bSSFP at rest and during exercise. For this approach, coil sensitivity maps were calculated from the temporal average of the input data in a central region of k-space, and image data were then reconstructed using a nonlinear iterative reconstruction with k-t regularization.2 Using incoherent sparse sampling, nonlinear reconstruction algorithms and iterative processing, 12-fold acceleration of image acquisition was achieved.3 This enabled whole heart coverage in one or two breath-holds (5-7s duration depending on heart rate), with in-plane spatial resolution of 2mm2 and temporal resolution in the order of 20ms. Typical parameters are presented in Table 1. All patients underwent an initial maximal cardiopulmonary exercise test (CPET) during supine cycle exercise to determine their maximal workload (workloadmax). Cine CS_bSSFP images were acquired in the left ventricular (LV) short axis and modified right ventricular (RV) short axis4 planes at rest and two pre-determined submaximal workloads (Rest: 0W, Ex1: 30% workloadmax and Ex2: 60% workloadmax) (Figures 1 & 2). In order to achieve steady-state exercise response, subjects cycled at each workload for 3 minutes prior to image acquisition. Between breath holds, subjects resumed cycling for 45s to return to steady-state exercise response. Typically, each subject would perform a total of 2 to 4 breath-holds at each workload (depending on heart rate response). Volumetric parameters were analysed using cvi42 software (Circle Cardiovascular Imaging, Calgary, Canada).Results
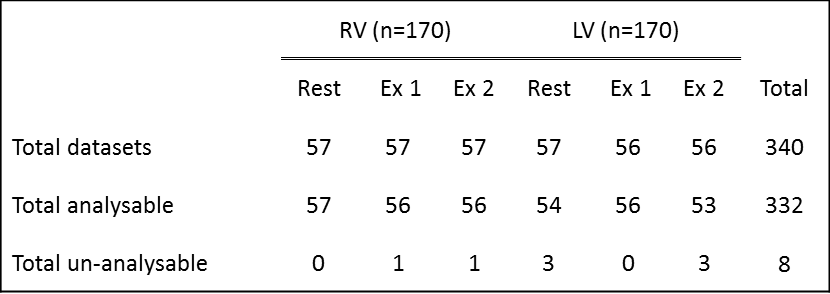
A total of 57 subjects (37 patients and 20 controls) with a mean age of 44 years (15-70 years) underwent exercise cardiac MRI. Exercise ergometry was well tolerated and the breath-holds were achievable at maximal exertion in all cases. A total of 340 ventricular datasets were acquired (114 at rest; 114 at Ex1; 112 at Ex2) (Table 2). Image quality was acceptable to enable volumetric analysis in 332 datasets. 8 were not acceptable for analysis due to patient-related ECG gating artefacts. No adverse events were encountered.Conclusions
Compressed sensing cardiac MRI for dynamic assessment of biventricular response during exercise is safe and highly feasible and permits dynamic quantitative ventricular functional analysis in a clinical setting.Acknowledgements
The authors would like to acknowledge Siemens Healthineers for provision of the prototype cine sequence and collaboration support.References
1. Attili AK, Schuster A, Nagel E, Reiber JH and van der Geest RJ. Quantification in cardiac MRI: advances in image acquisition and processing. The international journal of cardiovascular imaging. 2010; 26 Suppl 1: 27-40.
2. Jun Liu JR, Ti-chiun Chang, Alban Lefebvre, Michael Zenge, Edgar Mueller, Mariappan S. Nadar. Dynamic cardiac MRI reconstruction with weighted redundant Haar wavelets. ISMRM Scientific Meeting 2012.
3. Vincenti G, Monney P, Chaptinel J, et al. Compressed sensing single-breath-hold CMR for fast quantification of LV function, volumes, and mass. JACC Cardiovascular imaging. 2014; 7: 882-92.
4. Strugnell WE, Slaughter l R, Riley RA, Trotter AJ and Bartlett H. Modified RV short axis series--a new method for cardiac MRI measurement of right ventricular volumes. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2005; 7: 769-74.
Figures