4895
Accelerated, 3D Cine MRI with Stack of Stars k-space Sampling and Self-Navigation of Respiratory Motion for Aortic Valve Visualization.1Radiology, Northwestern University, Chicago, IL, United States, 2Biomedical Engineering, Northwestern University, Chicago, IL, United States, 3Cardiology, Northwestern University, Chicago, IL, United States
Synopsis
Aortic valve disease is the most common form of valvular heart disease in the western world and accurate aortic valve visualization is very important for this reason. Accurate imaging of the aortic valve is very critical in grading and diagnosing the severity of the disease. 3D imaging may enable better visualization of the aortic valve as compared to the standard 2D techniques due to both the ability to acquire high resolution volumetric coverage and to visualize in other imaging planes. This study describes the development and evaluation of an accelerated, 3D cine MRI pulse sequence using a combination of stack-of-star k-space sampling and XDGRASP reconstruction.
Introduction
Aortic valve disease is the most common form of valvular heart disease in the western world and accurate aortic valve visualization is very important for this reason. Aortic stenosis in particular has high morbidity and mortality and leads to complete heart failure unless the aortic valve replacement is performed. Other forms of aortic diseases such as aortic regurgitation, aortic ectasia, Marfan syndrome and aortic dissection are also fairly common. Accurate imaging of the aortic valve is very critical in grading and diagnosing the severity of the disease. 3D imaging may enable better visualization of the aortic valve as compared to the standard 2D techniques due to both the ability to acquire high resolution volumetric coverage and to visualize in other imaging planes.Methods
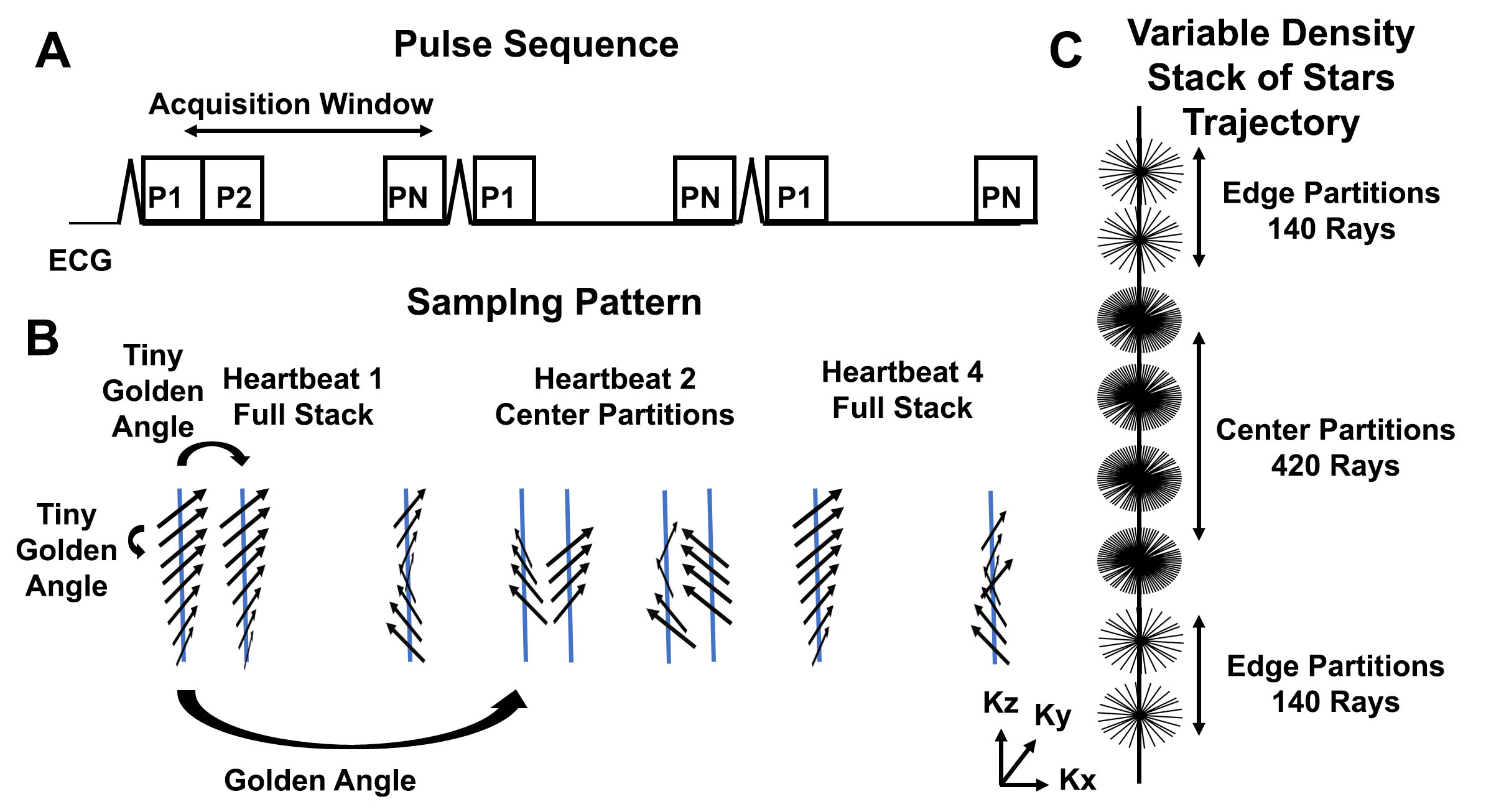
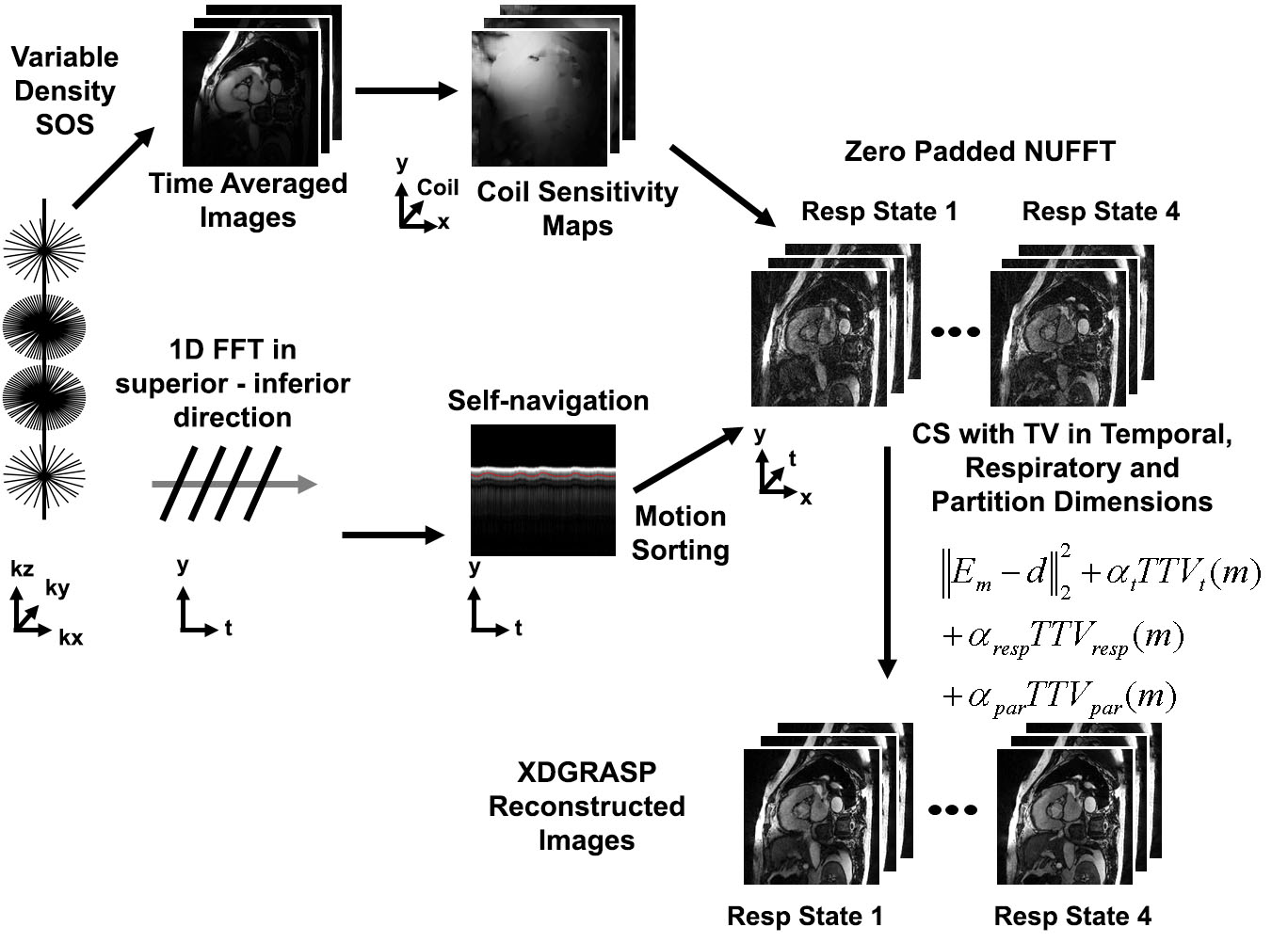
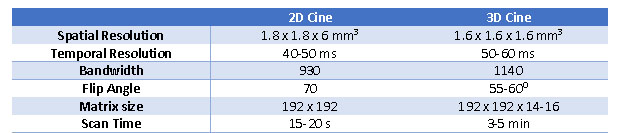
(Patients): We enrolled 7 patients (7 males and 5 females) who were scheduled to undergo a clinical cardiac MRI at 1.5T (Aera/Avanto, Siemens). (Pulse Sequence): We modified a b-SSFP pulse sequence with a stack-of-star k-space sampling to enable high resolution cine imaging. The pulse sequence (shown in Figure 1) employs a segmented variable density stack of stars k-space sampling1 where the center partitions are oversampled three times more than the outer partitions. In heartbeat one, a full stack is acquired followed by acquisition of two center stacks in the second heartbeat. The radial spokes are rotated by tiny golden angle2 along the partition and cardiac phase dimensions to produce more incoherent aliasing artifacts3. In each heartbeat, one ray in the center partition was oriented along the head-to-foot direction to track the respiratory motion, as previously described for XD-GRASP4. The proposed pulse sequence was used to perform a free breathing acquisition. Standard 2D cine imaging of the aortic valve was performed as a reference. Relevant imaging parameters for the 2D and 3D cine MRI sequences are summarized in Table 1. (Image Reconstruction): The reconstruction pipeline is shown in Figure 2. The k-space data were sorted into different respiratory states using a respiratory motion signal obtained from 1D FFT of ray acquired in superior-inferior direction. The reconstruction was performed in two steps. In step 1, XD-GRASP reconstruction was performed with 4 respiratory motion states using temporal total variance (TTV) as the sparsifying transform along the cardiac phase, respiratory and partition dimensions with normalized weights of 0.03, 0.01 and 0.01, respectively. In step two, two iterations of low-rank block-wise thresholding was performed to minimize the residual noise. (Data Analysis): Fourteen cine datasets (2 sets each for 7 patients) were randomized and evaluated by 2 readers in a blinded and independent manner using a 5-point Likert scale (1: worst; 3: clinically acceptable; 5: best) for the following four categories: conspicuity of the valve, artifact, temporal fidelity and noise. Wilcoxon signed rank test was used to compare the scores (p<0.05 was considered statistically significant).Results
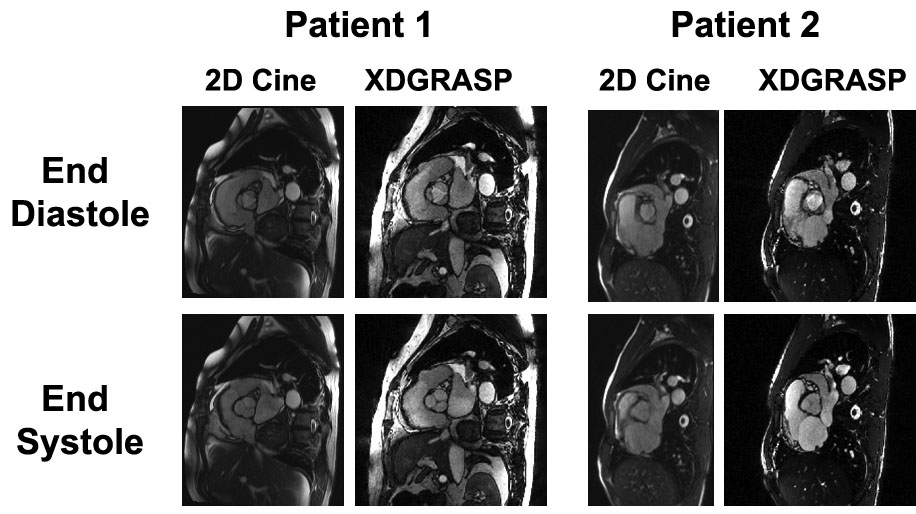
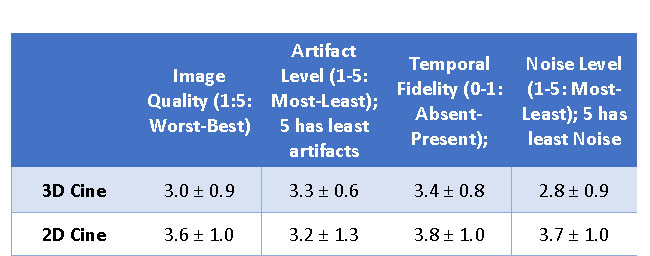
Figure 3 shows example cine images of the aortic valve at end-diastole and end-systole obtained using the standard 2D cine and free breathing 3D cine sequences in two different patients. As summarized in Table 2, the mean reader scores for all categories were not significantly different (p> 0.05).Conclusion
This study describes the development and evaluation of an accelerated, 3D cine MRI pulse sequence using a combination of stack-of-star k-space sampling and XDGRASP reconstruction. The visual assessment scores were not significantly different between the standard 2D and rapid 3D cine acquisitions. The proposed 3D method may be extended to provide more comprehensive evaluation of all the valves using a single acquisition without the need for breath holding. It may also be useful for applications where visualization of the valve is required at high resolution such as for TAVR planning.Acknowledgements
No acknowledgement found.References
1. Bhat H, Yang Q, Zuehlsdorff S, et al. Contrast‐enhanced whole‐heart coronary magnetic resonance angiography at 3 T with radial EPI. MRM. 2011 Jul 1;66(1):82-91.
2. Wundrak S, Paul J, Ulrici J, Hell E, Geibel MA, Bernhardt P, Rottbauer W, Rasche V. Golden ratio sparse MRI using tiny golden angles. Magn Reson Med 2016;75:2372–2378.
3. Zhou Z, Han F, Yan L, Wang DJ, et al., Golden-ratio rotated stack-of-stars acquisition for improved volumetric MRI. Magn Reson Med. 2017 Feb 6. doi: 10.1002/mrm.26625.
4. Feng L, Axel L, Chandarana H, Block KT, et al. XD‐GRASP: Golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. MRM. 2016; 75(2):775-88.
Figures