4894
Reconstructing real-time exercise stress cine images with multiple sets of sensitivity maps1The Ohio State University, Columbus, OH, United States
Synopsis
Motivated by the changing sensitivity maps due to exaggerated chest wall motion in real-time stress cardiac MRI (CMR), we utilize ESPIRiT-based multiple sets of sensitivity maps in a SENSE-based reconstruction method to reduce image artifact. The proposed method was tested on twelve volunteers and compared with the images reconstructed using a temporally invariant single set of sensitivity maps as well as a temporally varying single set of sensitivity maps. It was demonstrated that using multiple sets of sensitivity maps leads to significant reduction in image artifact.
Background
Method
A nine-slice stack of short axis real-time cine images covering the left ventricle was acquired in twelve healthy volunteers immediately following maximal exercise to exhaustion on an MRI compatible treadmill positioned next to the MRI patient table. The protocol information on a 1.5T scanner (Avanto, Siemens Healthcare, Erlangen, Germany) was: FOV 350-420mm, TE/TR 1.02/2.34ms, image matrix 192x126, flip angle 60 degrees, acceleration rate 9 using VISTA sampling pattern [2], spatial resolution ~2.5x2.2mm2, temporal resolution 33ms.
Images were reconstructed using a SENSE-based CS method with auto-tuning of regularization parameters [3]. Cardiac frames were averaged to generate ACS lines, and ESPIRiT was used to estimate the coil sensitivity maps. When using multiple sets of sensitivity maps, the strict SENSE model was extended to “soft” SENSE reconstruction, where the signal in k-space was represented in terms of multiple sets of images, each with its own set of sensitivity maps. The final reconstructed image was the sensitivity map-weighted sum of all sets of images [1].
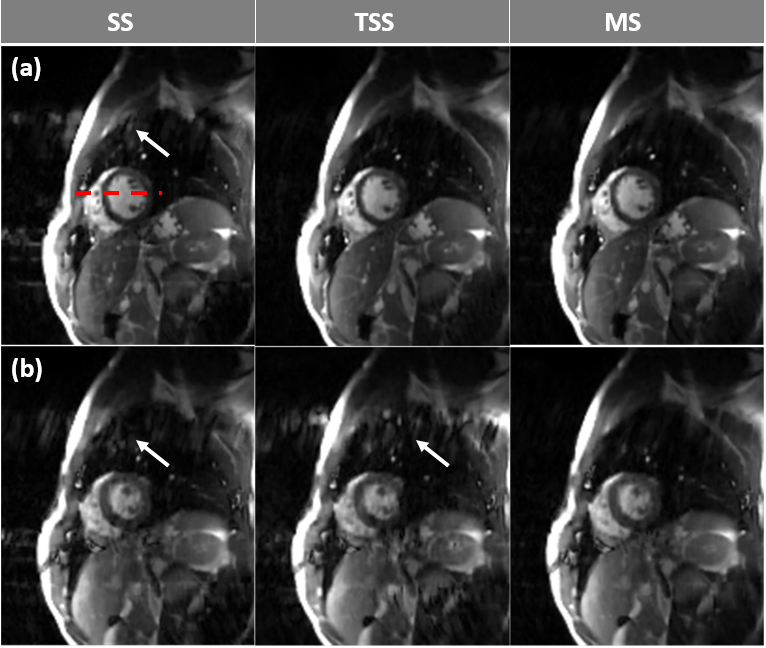
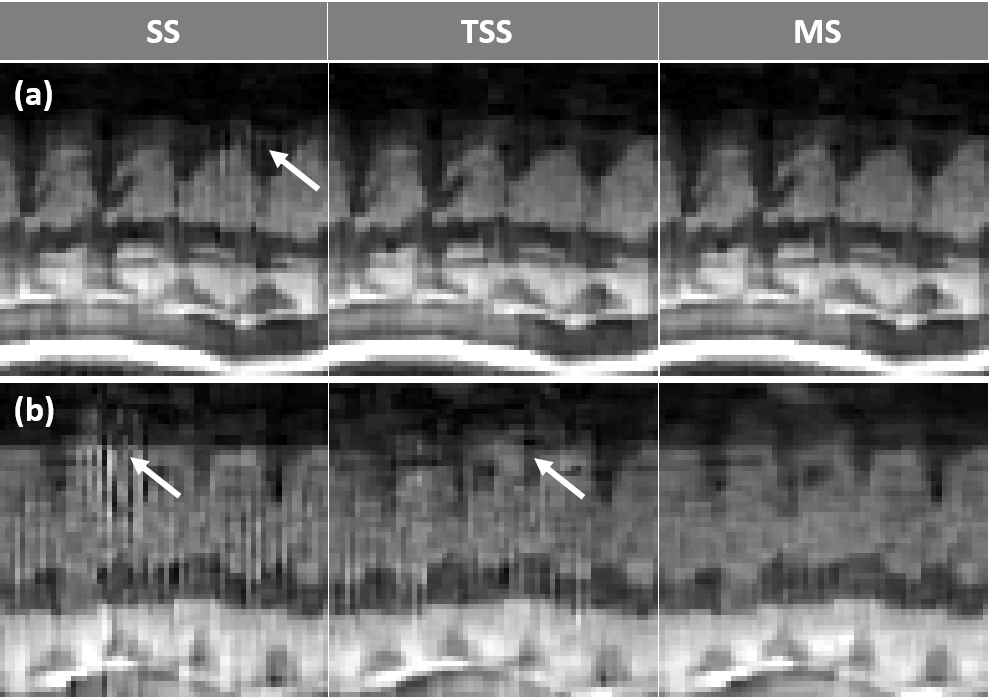
As a comparison, we reconstructed the images using three different sensitivity maps: a single set of sensitivity maps (SS), a single set of temporally varying (respiratory phase specific) sensitivity maps (TSS), and temporally invariant multiple sets of sensitivity maps (MS). One and three sets of sensitivity maps were estimated for SS and MS, respectively, using the ACS lines generated by averaging undersampled k-space data from all cardiac frames. For TSS, one set of sensitivity maps was estimated from ACS lines generated by averaging undersampled k-space data from 17 consecutive frames, yielding temporally varying sensitivity maps. Finally, all the reconstructed images were visually scored in terms of the level of artifacts (1: no artifact; 2. minor artifact; 3. significant artifact but diagnostic; 4. severe artifacts but barely diagnostic; 5. non-diagnostic due to extreme artifacts).
Results and Discussion
Conclusion
Acknowledgements
This work was partially funded by NIH grant R01HL135489.References
[1] Uecker, M. et al. Magnetic Resonance in Medicine 71 (3), 990–1001 (2014).
[2] R. Ahmad. et al. Magnetic Resonance in Medicine 74 (5), 1266-1278 (2015).
[3] R. Ahmad. et al. IEEE Transactions on Computational Imaging 1 (4), 220-235 (2015).
Figures