4891
A comparison of motion compensated spin echo (M2SE) and stimulated echo acquisition mode (STEAM) diffusion tensor cardiovascular magnetic resonance in the in vivo assessment of hypertrophic cardiomyopathy.1CMR Unit, Royal Brompton Hospital, London, United Kingdom, 2National Institutes of Health, Bethesda, MD, United States
Synopsis
Diffusion tensor cardiovascular magnetic resonance (DT-CMR) interrogates myocardial microstructure, using parameters such as mean diffusivity (MD), fractional anisotropy (FA) and secondary eigenvector angulation (E2A), an index of sheetlet orientation. We compared motion compensated spin echo (M2SE) and stimulated echo acquisition mode (STEAM) and their ability to distinguish hypertrophied fibrosed myocardium (LVH+Gd+) in hypertrophic cardiomyopathy.
M2SE discriminated areas of LVH+Gd+ best through FA and MD, whilst STEAM was more sensitive to changes in E2A mobility. FA derived from both M2SE and STEAM correlated significantly with extracellular volume.
Introduction
Diffusion tensor cardiovascular magnetic resonance (DT-CMR) interrogates the myocardial microstructure, providing a novel method of phenotyping. DT-CMR parameters include mean diffusivity (MD), fractional anisotropy (FA) and the absolute secondary eigenvector angulation (E2A), a DT-CMR measure of sheetlet orientation. Two frequently used DT-CMR techniques are motion-compensated spin echo (M2SE) and stimulated echo acquisition mode (STEAM). Whilst M2SE is strain insensitive and SNR efficient, STEAM has a longer mixing time and does not require motion compensation. STEAM has detected abnormalities in the microstructure of hypertrophic cardiomyopathy (HCM) patients. Diastolic E2A is significantly elevated in HCM compared to controls, suggesting a failure of diastolic relaxation of sheetlets1. We have previously evaluated both M2SE and STEAM in HCM, showing both identify abnormally elevated diastolic E2A compared to controls. M2SE provides higher MD and lower FA measures, due to the shorter mixing time2. We develop this work, exploring whether both DT-CMR techniques discriminate hypertrophied fibrosed myocardium in HCM and whether DT-CMR parameters correlate with fibrosis, measured by extracellular volume (ECV).
Methods
Ten HCM patients had DT-CMR and late gadolinium (Gd) imaging at 3T (Siemens, Skyra) in a mid-ventricular short axis slice. STEAM and M2SE data were acquired using bmain=450smm-2 and bref =150smm-2, in 6 directions with voxel size of 2.8x2.8x8mm3 (1.4x1.4x8mm3 reconstructed), SENSE x2, field of view 360x135mm2. STEAM imaging used TE=23ms, TR=2RR-intervals (7 images per breath hold) and SE imaging used TE=75ms, TR=1RR-interval (14 images per breath hold). A minimum of 8 STEAM or 16 M2SE averages of satisfactory quality were acquired at both end systole and diastasis. The slice was divided into 12 segments, where the first contained the superior insertion point. Segments were visually segregated into regions of hypertrophy (LVH+) and late gadolinium enhancement (Gd+) and those with neither (LVH-Gd-) by an experienced operator. DT-CMR data were processed using custom MATLAB software. Diffusion parameters were compared between LVH+Gd+ and LVH-Gd- areas, and also correlated to ECV.Results
Demographics were 7/10 male, median[IQR] age 64[11] years. Median maximum wall thickness was 20[5]mm, ejection fraction was 76[3]%. All patients had septal hypertrophy and septal fibrosis; median gadolinium enhancement was 1.5[2.9]g, at 5.2[13]% of the slice. Two M2SE diastole datasets were rejected for poor-quality due to mis-triggering and bulk motion signal loss. Figure 1 shows examples of good quality and rejected data. Table 1 shows biphasic global diffusion parameters obtained by M2SE and STEAM and their relative difference. M2SE sequences generated biphasic higher MD and lower FA.
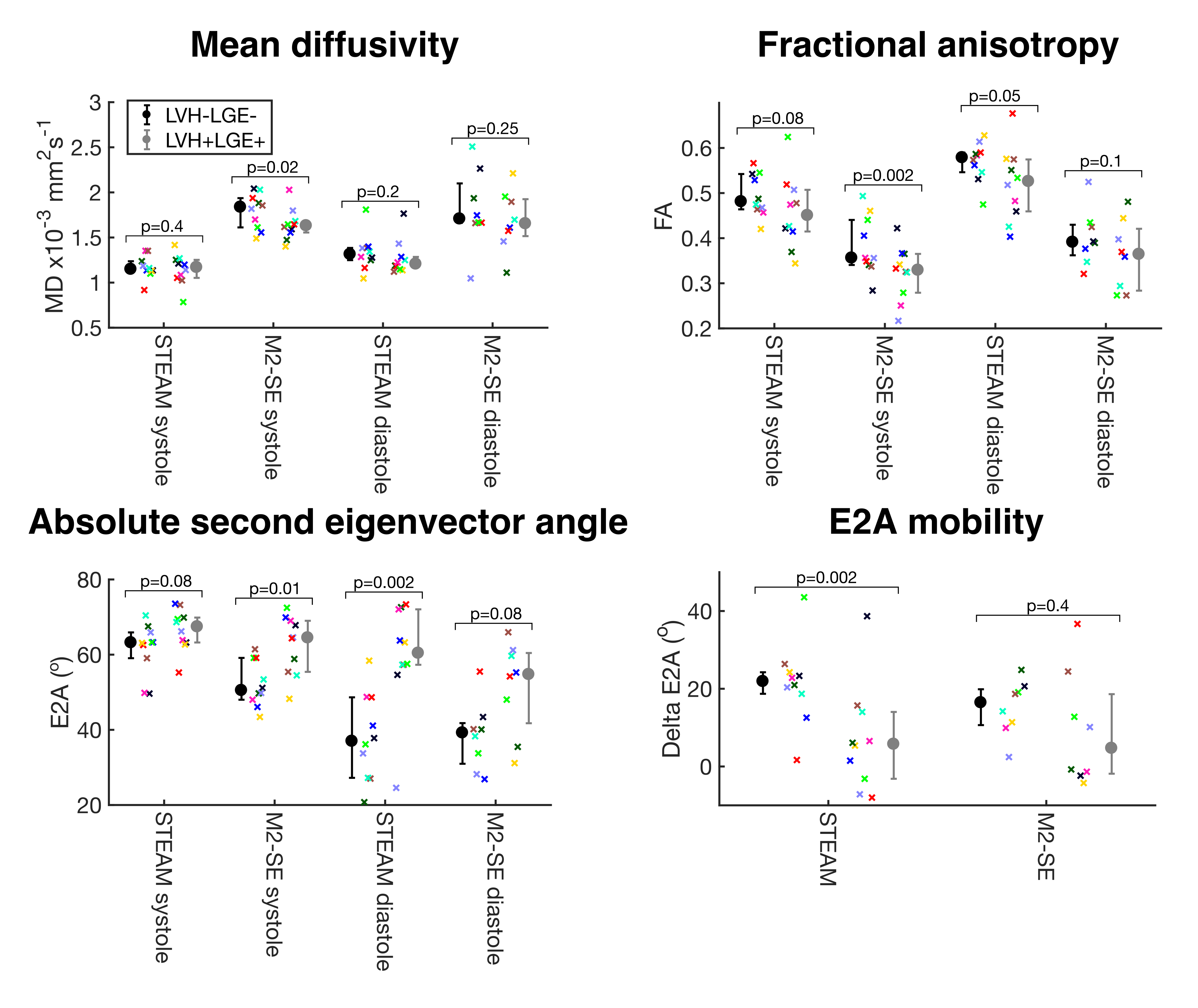
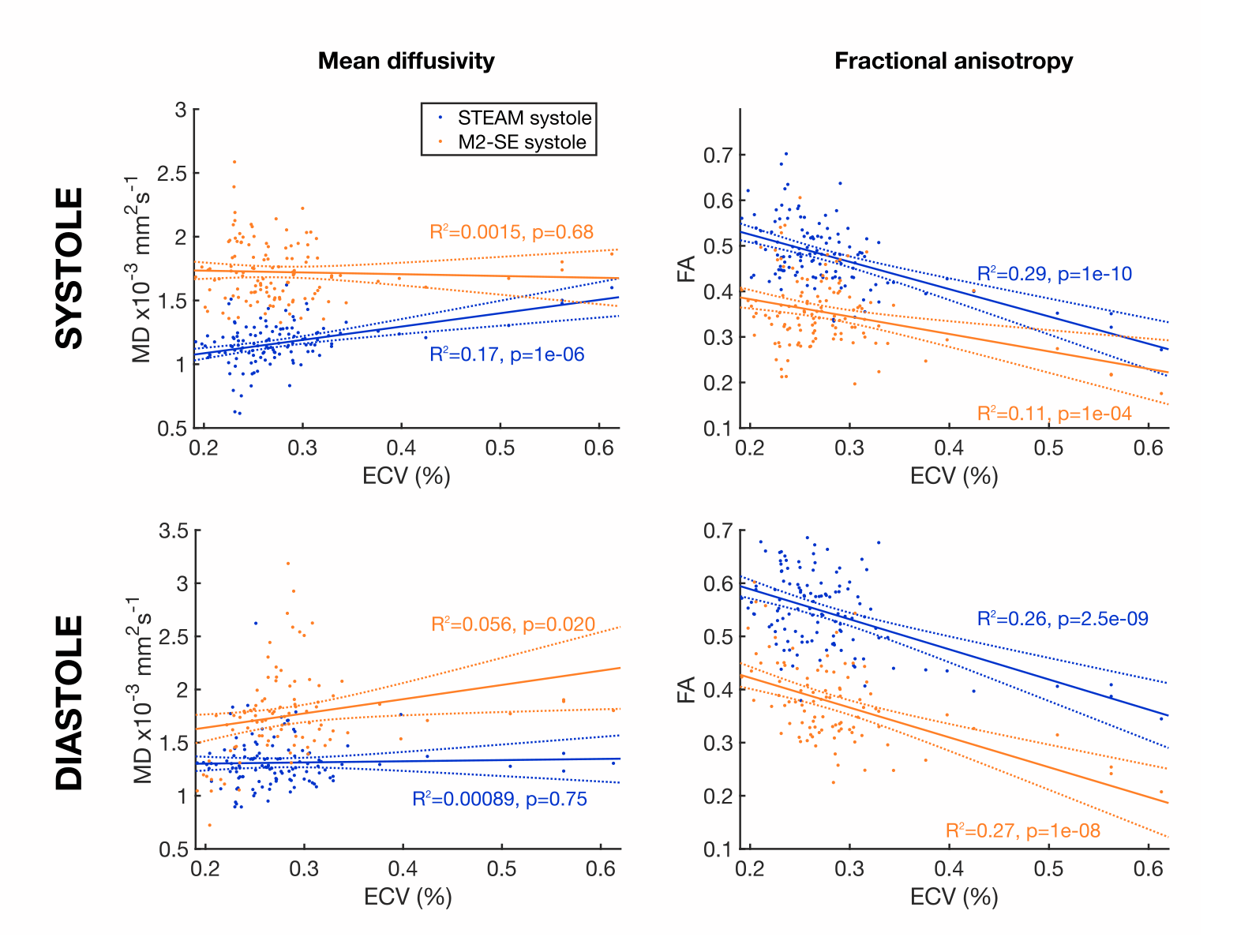
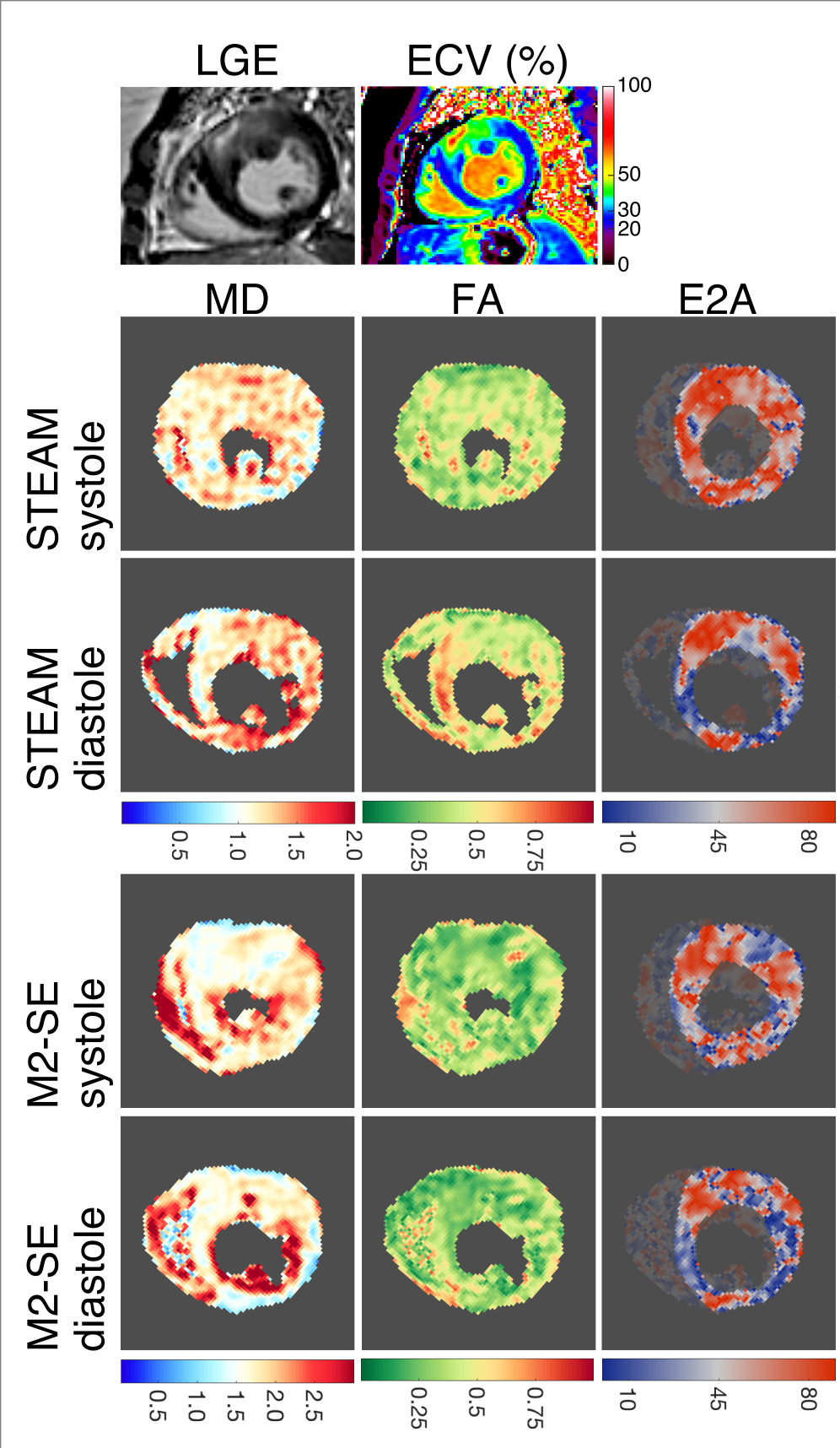
Figure 2 shows diffusion measurements assessed by M2SE and STEAM, segregated by LVH+Gd+ and LVH-Gd-. For MD and FA in diastole M2SE and STEAM were comparable. In systole only M2SE found differences in LVH+Gd+ vs LVH-Gd- (MD 1.63[0.13] vs 1.84[0.32] x10-3mm2/s, p=0.02 and FA 0.329[0.086] vs 0.356[0.100], p=0.002). LVH+Gd+ segments had higher E2A than non-affected segments in both techniques, but this was only significant by M2SE in systole and STEAM in diastole. However, only STEAM is able to discriminate between LVH+Gd+ and LVH-Gd- areas by E2A mobility. Figure 3 shows MD and FA correlated with ECV at both cardiac phases. FA correlates with ECV: as ECV rises, FA falls with p < 0.001.Figure 4 shows example DT-CMR parameter maps and the corresponding Gd and ECV maps, with reasonable correspondence between the region of Gd, ECV and E2A.
Discussion
Both M2SE and STEAM are feasible in the assessment of HCM. M2-SE discriminates between LVH+Gd+ and LVH-Gd- areas using FA and MD, but only in systole. We demonstrated decreased MD in hypertrophied fibrosed areas. A previous diffusion-weighted study has shown increased MD in areas of fibrosis in HCM, but FA was not assessed3. However DT-CMR can assess FA, and showed the expected reduction in areas of hypertrophied fibrosis, with correlation to ECV. For E2A and E2A mobility STEAM was the better discriminator between LVH+Gd+ and LVH-Gd- areas, with elevated diastolic E2A and reduced E2A mobility in keeping with the proposed mechanism of failure of diastolic relaxation in HCM1.Conclusion
STEAM appeared to be more sensitive to the detection of sheetlet function abnormalities in phenotypically affected myocardium, whilst M2SE may be more sensitive for detecting markers of disorganisation.Acknowledgements
We would like to thank Mr Rick Wage for his expert technical help.References
1. Ferreira PF, Kilner PJ, McGill L-A, Nielles-Vallespin S, Scott AD, Ho SY, et al. In vivo cardiovascular magnetic resonance diffusion tensor imaging shows evidence of abnormal myocardial laminar orientations and mobility in hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2014;16(1):87
2. Khalique Z, Scott AD, Ferreira PF, Gorodezky M, Wage R, Nielles-Vallespin S, Firmin DN, Pennell DJ. An initial evaluation of STEAM and M012 spin echo diffusion tensor imaging in hypertrophic cardiomyopathy patients. 20th Annual SCMR Scientific Sessions Abstract Supplement, Washington DC, USA 2017
3. Nguyen C, Lu M, Fan Z, Bi X, Kellman P, Zhao S, et al. Contrast-free detection of myocardial fibrosis in hypertrophic cardiomyopathy patients with diffusion-weighted cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2015;17:107.
Figures
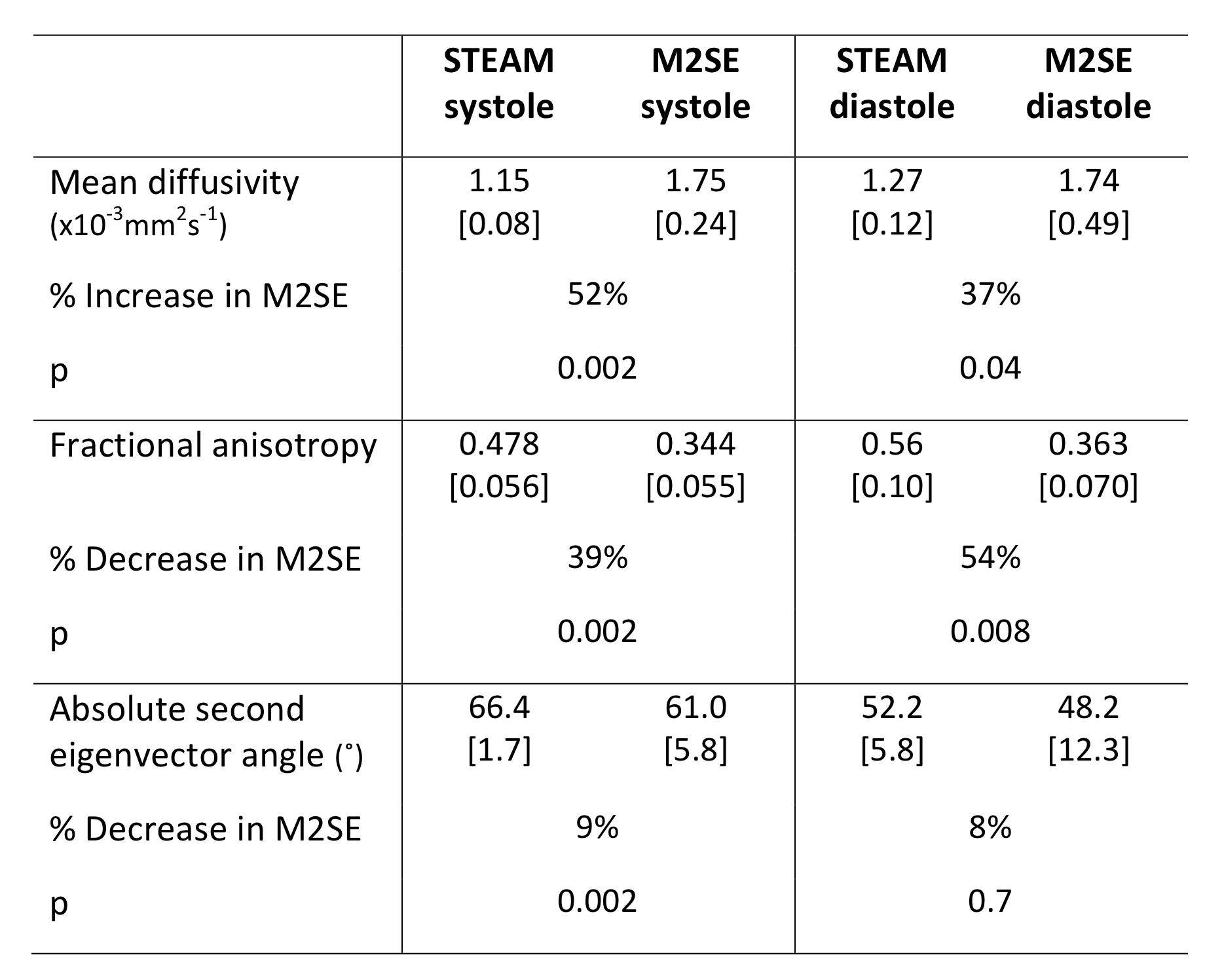
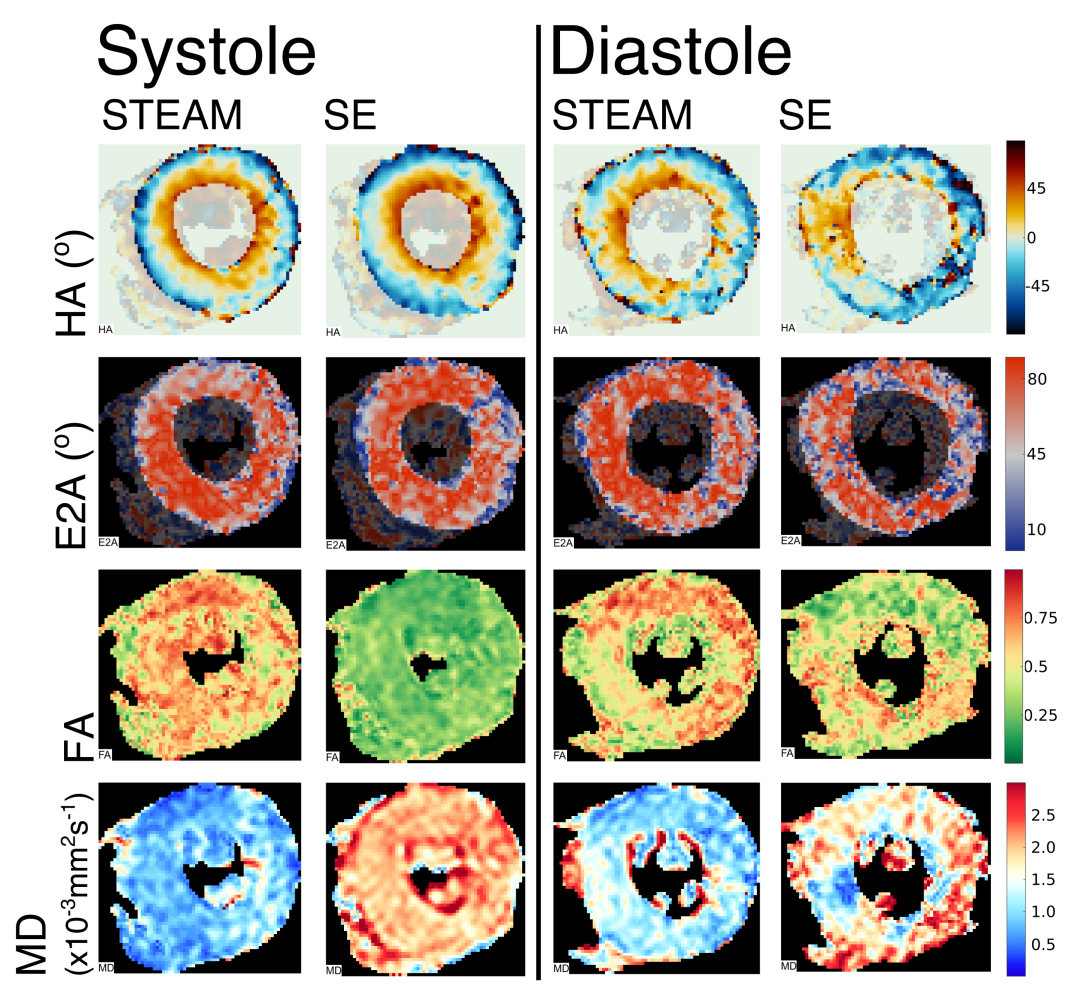
Figure 1: Examples of acceptable maps and rejected maps.
Maps of helix angle (HA), secondary eigenvector angulation (E2A), fractional anisotropy (FA) and mean diffusivity (MD) at both systole and diastole using stimulated echo acquisition mode and spin echo (SE). Systolic maps were accepted, but the diastolic SE map was rejected.