4880
Feasibility Study of Whole Heart T1 Mapping with SMS in A Single Breath HoldWenbo Sun1, Meng Ye2, Yuan Zheng3, Lele Zhao2, Nan Liu2, Yanqun Teng2, Lan Lan1, Jian Xu3, and Haibo Xu1
1Department of Radiology, Zhongnan Hospital of Wuhan University, Wuhan, China, 2United Imaging Healthcare, Shanghai, China, 3UIH America Inc., Houston, TX, United States
Synopsis
A novel single breath
hold (BH) whole-heart T1 mapping technique with simultaneous multi-slice (SMS) imaging
with improved spatial coverage and faster acquisition speed is proposed and evaluated,
the initial results show that the proposed whole heart T1 mapping approach has
similar results compared to conventional approaches.
Introduction
Myocardial T1 mapping is of high importance for the detection of diffuse fibrosis and other myocardial diseases. Many techniques have been proposed for myocardial T1 mapping, The Modified Look-Locker Inversion recovery (MOLLI) method is the most widely used one for its precision and stability [1], however, this method can only acquire one single slice T1 map in each BH. Recently, a whole heart T1-mapping method was proposed to cover the whole heart, which generates T1 maps of 9 slices in a single BH [2], however, limited by the image acquisition speed, the 9 T1 maps were not in the same cardiac phase and were not enough to cover the entire heart. Another T1 mapping approach was introduced using simultaneous multi-slice (SMS) imaging technique based on MOLLI approach [1], which can only cover 1 to 3 slices of the heart in a single BH [3]. In this study, we propose a novel single BH whole-heart T1 mapping technique using SMS technique with improved spatial coverage and faster acquisition speed in which every slice was acquired at the same cardiac phase within one single BH.Methods and Materials
To achieve whole heart covered and rapid T1 mapping, a modified saturation recovery (SR) prepared pulse sequence was implemented with SMS technique using balanced steady state free precision (bSSFP) readout kernel, the images were then reconstructed using the slice-GRAPPA algorithm [4] [5].The Schematic pulse sequence diagram of the whole heart T1-mapping is illustrated in Fig. 1, in the first N heart beats (HB) , number N slices of proton density weighted (PDw) images were acquired at a time delay (TD) plus a time inversion (TI) after the R wave without SR preparation. In the following N HBs, corresponding number N slices of T1-weighted images (T1w) were acquired at TD + TI after the R wave with SR preparation. Phantom and in vivo whole heart T1 mapping was performed using a 3T MRI scanner (uMR 770, UIH, Shanghai, China) with a 12-channel body array coil. The parameters were: slice number = 12, slice thickness = 7 mm, slice gap= 50%, FOV = 360 × 300mm, matrix = 256 × 75, flip angle = 70°, TR = 3.1ms, TE = 1.5ms, band width = 1500 Hz/Pixel. For fair comparisons, images with above mentioned parameters except the multi band factor (MB) =1 (Method 1) and 2 (Method 2) were acquired separately, T1 mapping of each method was calculated from a pair of images from the PDw and T1w of the same slice using the equation of [2]. The results from Method 1 were also served as the reference data needed in the SMS reconstruction in method 2.Results
Fig. 2 shows the results of PDw, T1w and T1 maps of the phantom acquired with Method 1 (top) and Method 2 (bottom). Compared to Fig.2(c), Fig.2 (f) shows some artifacts in the phase encoding direction. Fig. 3 demonstrates the results of PDw, T1w and T1 maps of whole heart from one healthy subject (32 years old, male). The T1 maps calculated from Method 1 and Method 2 are similar and consistent with the empirical value (T1 of ~1s at 3.0T). Compared to Method 1, the total scan time of Method 2 was in half of the time of method1, about 9.6 seconds, which is acceptable for routine clinic application, While Fig.3 (b) shows more motion artifacts compared to Fig.3 (e), due to the long BH time of Method 1. These results indicate that the proposed approach enables accurate and rapid whole heart T1 mapping.Conclusions
Conventional T1 mapping is time consuming and usually does not cover the whole heart, which might cause patient discomfort and image misalignment. The proposed whole heart T1 mapping approach with SMS could considerably reduce the total scan time. We have demonstrated that with MB factor = 2, whole heart T1 maps of 12 slices at the same cardiac phase can be acquired within one single BH and the initial results show that similar T1 maps can be achieved from this proposed approach. A clinical evaluation of myocardial fibrosis and other myocardial disorders using this proposed approach is under the way.Acknowledgements
No acknowledgement found.References
[1] Messroghli DR, et al. Magn Reson Med. 2004 Jul;52(1):141-146.
[2] Sohae C, et al. J Cardiovasc Magn Reson. 2015;17(S1):389
[3] Weingartner S, et al. J Cardiovasc Magn Reson. 2017 Aug;78(2):462-471.
[4] Yuan Z,et al. ISMRM 2017 p1271.
[5] Xiaoqian H, et al. Chinese Journal of Magnetic Resonance, 2017,34(3):283-203.
Figures
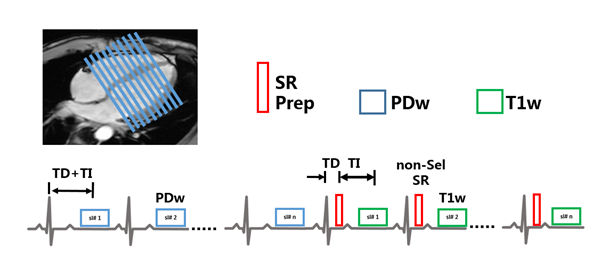
Figure 1 Schematic pulse
sequence diagram of the whole heart T1-mapping, a number of paired PDw without
SR and T1w with non-selective SR images acquired at the same cardiac phase.
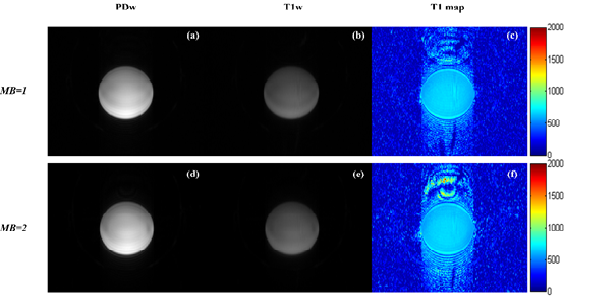
Figure 2 One slice image
of a phantom acquired with MB=1 (a-c) and MB=2 (d-f), (a) (d): images without saturation
pulse, (b) (e): images with non-selective saturation pulse, (c) (f): calculated
T1 maps. Some artifacts in the phase encoding direction due to g-factor of the
RF coil.
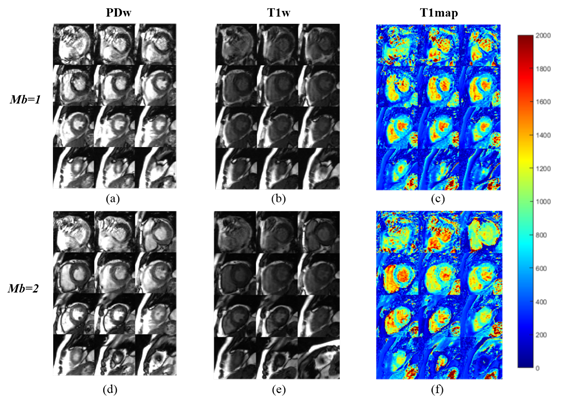
Figure 3 Whole heart
images of total 12 slices (24 images) acquired with MB=1 (top) and MB=2
(bottom) separately, which cover the entire heart from apex to basal :( a) (d):
PDw without SR, (b) (e): T1w images with non-selective SR, (c) (f): calculated
T1 maps. The T1 maps calculated from Method 1 and Method 2 are similar and consistent
with the empirical value (T1 of ~1s at 3.0T).