4876
Myocardial Oxygenation Using T2* BOLD Cardiac MRI with Compressed SENSE: Association with Myocardial Fibrosis and Contraction in Hypertrophic Cardiomyopathy1Diagnostic Imaging & Nuclear Medicine, Tokyo Women's Medical University, Tokyo, Japan, 2Cardiology, Tokyo Women's Medical University, Tokyo, Japan, 3Radiological service, Tokyo Women's Medical University, Tokyo, Japan, 4Philips Electronics Japan, Tokyo, Japan
Synopsis
We developed a new method for myocardial oxygenation using oxygen-inhalation blood-oxygen-level-dependent (BOLD) T2* cardiac magnetic resonance imaging (T2*-CMR). Myocardial oxygenation (ΔR2*, ms-1) was defined as the difference in R2* between under room-air and oxygen inhalation. ΔR2* is increased in patients with hypertrophic cardiomyopathy who had large LGE areas and low strains, suggesting that impairment of myocardial oxygenation associates with myocardial fibrosis and systolic dysfunction. In addition, T2*-CMR with compressed SENSE enables to shorten scan time and less motion artifact. This contributes to make high precision of T2* and R2* maps.
Purpose
Recently, we developed a new analytic technique for myocardial oxygenation using oxygen-inhalation blood-oxygen-level-dependent (BOLD) T2* cardiac magnetic resonance imaging (T2*-CMR). In refractory heart failure, ΔT2* (T2*oxy-T2*air) is correlated with oxygen metabolism during exercise as measured by CPX test (1). Myocardial fibrosis presented as late gadolinium enhancement (LGE) area has the prognostic value in clinical outcome for hypertrophic cardiomyopathy (2). Decreased myocardial strain is used as standard of systolic dysfunction (3). The present study investigates whether myocardial oxygenation derived from T2*-CMR associates with myocardial fibrosis and contraction in patients with hypertrophic cardiomyopathy.Methods
Data of CMR (Inginia 3T Quasar Dual; Philips Healthcare) equipped with dual-source parallel radiofrequency transmission, 32-element cardiac phased-array coils, and cardiac gating with a 4-lead vector electrocardiogram for 20 patients with hypertrophic cardiomyopathy was analyzed. T2*-CMR was accomplished using the black blood, breath-hold, and multi-echo gradient-echo sequence (TE=2.3 to 16.4 ms) with compressed SENSE. T2* and R2* maps were automatically calculated by fitting the signal intensity data for the mid-left ventricular septum to a decay curve using a special software named for Star-Quant (Fig. 1). During 10 minutes inhalation of oxygen at the flow rate of 10 l/min, R2* was measured under room-air and after oxygen inhalation. Myocardial oxygenation (ΔR2*, ms-1) was defined as the difference between the two conditions. The LGE area was determined by a threshold of 6 SD above the mean signal intensity of remote normal myocardium (4). The summed LGE volume (cm3) per a patient was measured and used as an estimate of myocardial fibrosis (Fig. 2). Circumferential myocardial strain (%) was obtained from high-temporal cine-tagging imaging of the short-axis of the mid-left ventricle using TFEPI grid pulse with 50 phases per cycle (5) (Fig. 3). Comparison of ΔR2* between divided two groups by the means of the summed LGE area and circumferential strain was analyzed by the Mann-Whitney u-test.Results
The mean LGE area and circumferential stain were 18 cm3 and 10.5%, respectively. The patients were divided into two groups with LGE area >18cm3 and <18cm3, and with circumferential strain >10.5% and <10.5%. ΔR2* was significantly greater for patients with LGE area >18cm3 than those with LGE area <18cm3 (19.3±9.7 vs. 5.6±4.9ms-1,p<0.05). ΔR2* was significantly greater for patients with circumferential strain <10.5% than those with circumferential strain >10.5% (16.5±13.9 vs. 6.4±4.5ms-1, p<0.05). R2* maps for representative case with diffuse fibrosis and small strains are presented in Figure 4.
Discussion
1. BOLD effect to myocardium. The increased oxy-hemoglobin with increasing blood volume is proportional to the elevation of tissue T2* value, meaning BOLD effect. Oxygen inhalation affects to decrease coronary flow and the elevation of coronary vascular resistance. Consequently, oxy-hemoglobin reduces in the impaired tissue. On the other hand, active inflammation and edema in cardiomyopathy effect to increased blood volume. This leads to increase oxy-hemoglobin. These reverse changes in oxy-hemoglobin causes unstable T2* and R2* values in the injury myocardium.
2. Advantage of Star-Quant T2*-CMR with Compressed SENSE. Compressed SENSE enables to shorten scan time, resultantly it can reduce motion artifact on T2* image with long echo times (Fig. 5). This contributes to make high precision of T2* and R2* maps.
Conclusion
Star-Quant T2*-CMR with compressed
SENSE is a noninvasive and feasible method for the quantification of myocardial
oxygenation. ΔR2* is increased in patients with hypertrophic cardiomyopathy who
had large LGE areas and low strains, suggesting that impairment of myocardial
oxygenation associates with myocardial fibrosis and systolic dysfunction.
Acknowledgements
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (16K10321).References
1. Nagao M, Yamasaki Y, Kawanami S, et al. Quantification of myocardial oxygenation in heart failure using blood-oxygen-level-dependent T2* magnetic resonance imaging: comparison with cardiopulmonary exercise test. Magn Reson Imaging 2017: 39; 138-143.
2. Green J, Berger JS, Karmer CM, Salerno M. Prognostic value of late gadolinium enhancement in clinical outcomes for hypertrophic cardiomyopathy. JACC Cardiovasc Imaging 2012: 5; 370-377.
3. Nagao M, Yamasaki Y, Yonezawa M, et al. Geometrical characteristics of left ventricular dyssynchrony in adverse heart failure: myocardial strain analysis by tagged MRI. Int Heart J 2014: 55; 512-518.
4. Rayatzadeh H, Tan A, Chan RH, et al. Scar heterogeneity on cardiovascular magnetic resonance as a predictor of appropriate implantable cardioverter defibrillator therapy. J Cardiovasc Magn Reson 2013: 15; 31
5. Yamasaki Y, Nagao M, Abe K, et al. Balloon pulmonary angioplasty improves interventricular dyssynchrony in patients with inoperable chronic theomboembolic pulmonary hypertension: a cardiac MR imaging study. Int J Cardiovasc Imaging 2017: 33; 229-239.
Figures
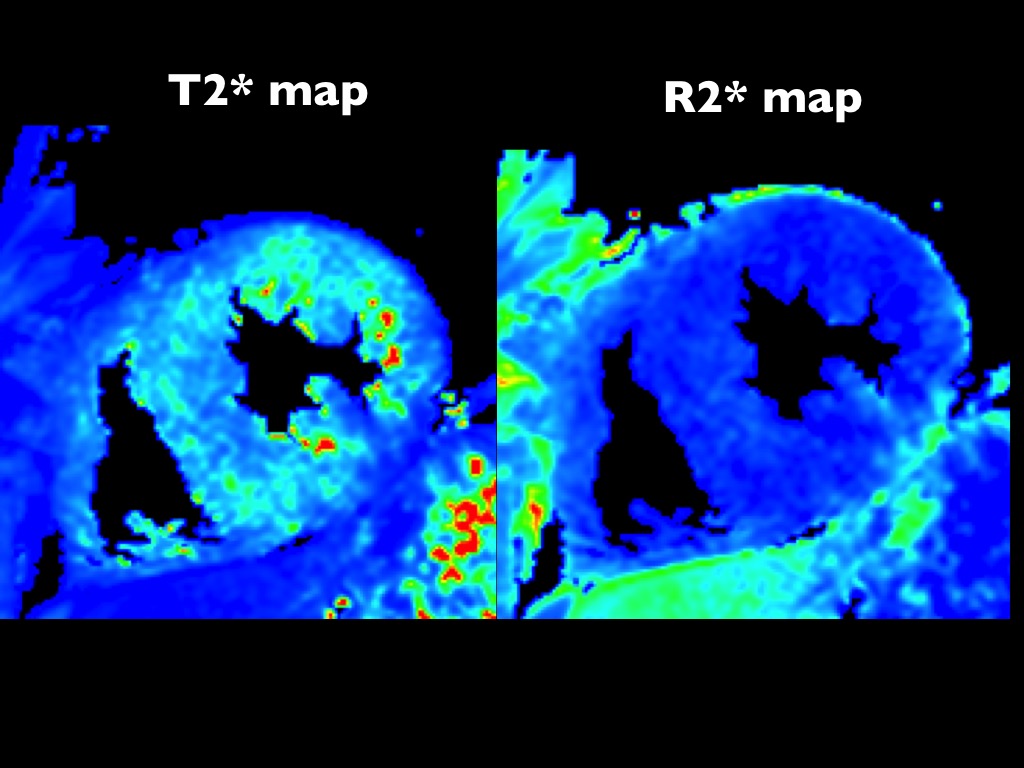
Figure 1. T2* and R2* maps.
T2* and R2* maps are automatically reconstructed using a special software named for “Star-Quant”. R2* map has less noise than T2* map.
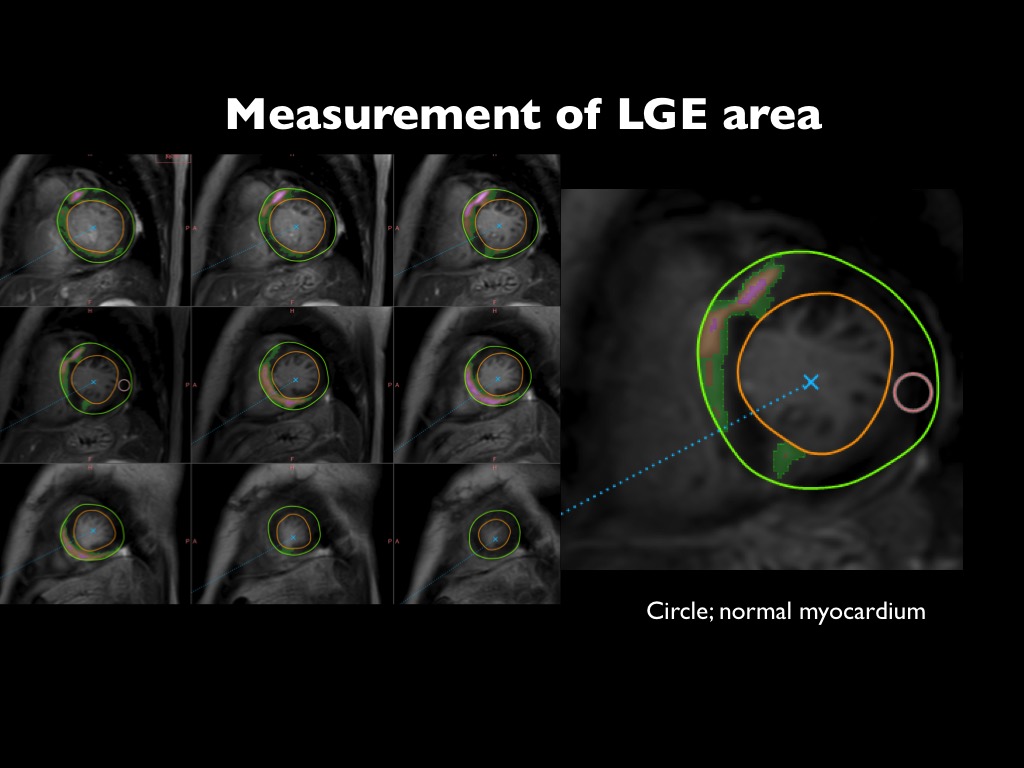
Figure 2. Quantification of LGE.
LGE area was determined using a threshold of 6SD above the mean of remote normal myocardium. The amount of LGE volume was measured. Green and pink colored areas correspond to LGE areas. Circle (right) is referenced as normal myocardium.
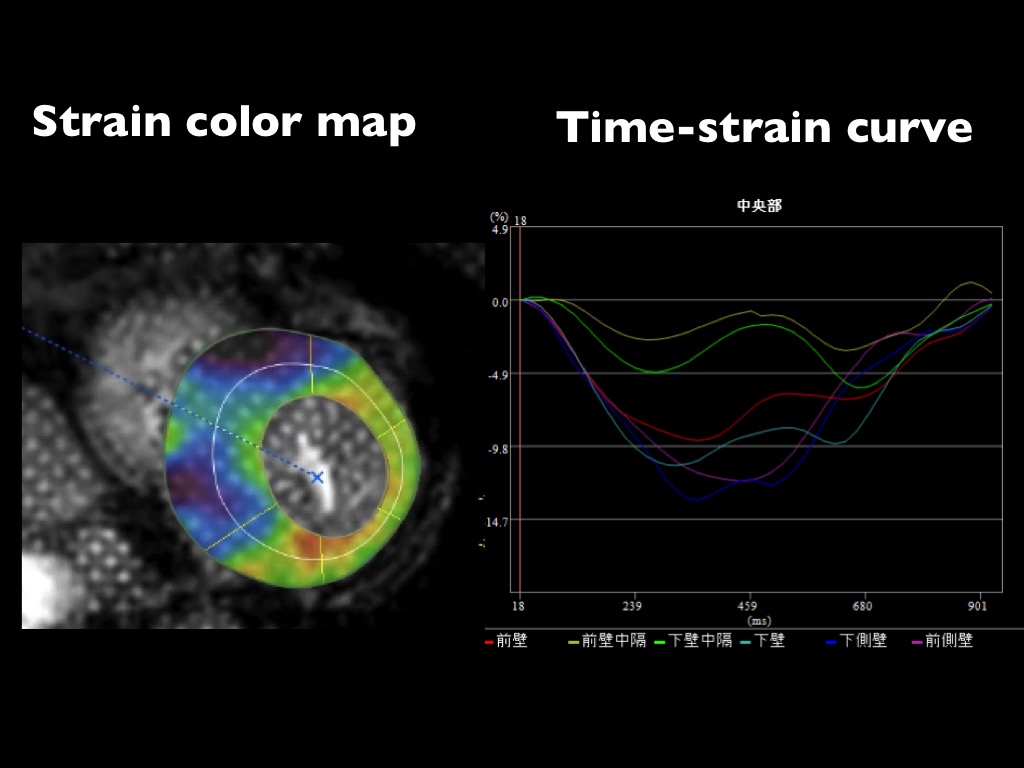
Figure 3. High-temporal tagging imaging.
High-temporal tagging imaging using TFEPI with a resting grid pulse shows colored circumferential strain (left). Time-curves of circumferential strain for 6 myocardial segments are analyzed by available software named for “Phyziodynamics” (Ziosoft Co.) (right).
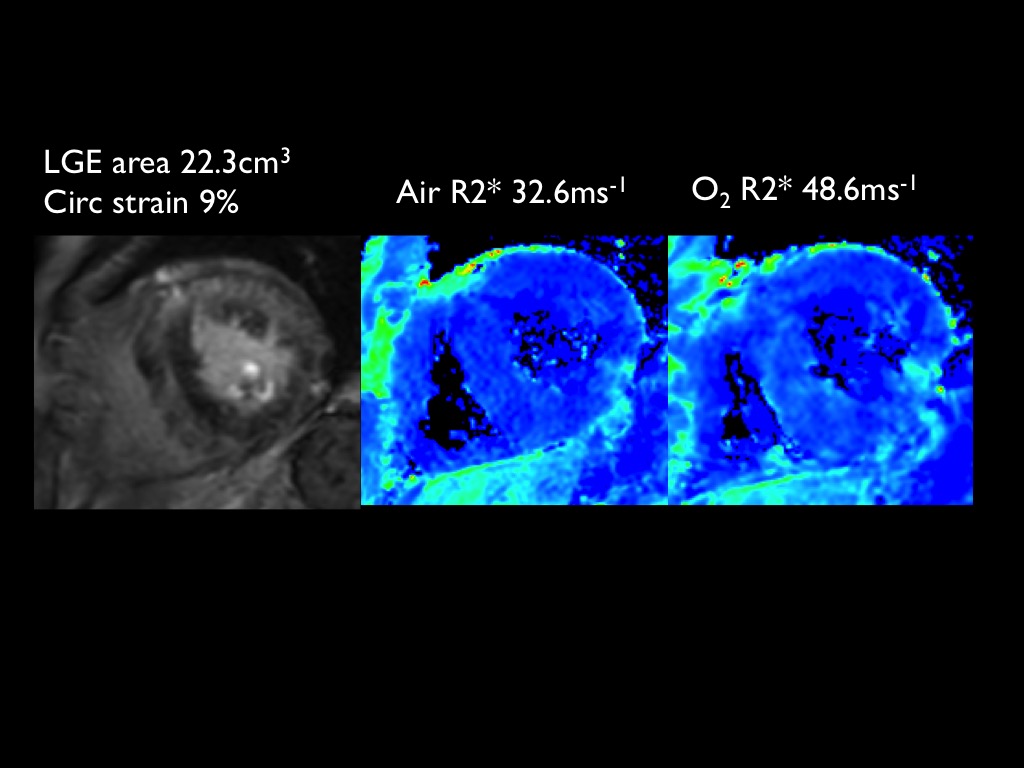
Figure 4. 50s man with hypertrophic cardiomyopathy.
LGE MRI shows diffuse myocardial fibrosis (LGE area, 22.3cm3) in the left ventricle (left). His circumferential strain is low (9%). R2* map after oxygen inhalation shows increased signal intensity (48.6msec-1) in the septum, compared with that under room air (32.6msec-1). ΔR2* of 16msec-1 suggests impairment of myocardia oxygenation.
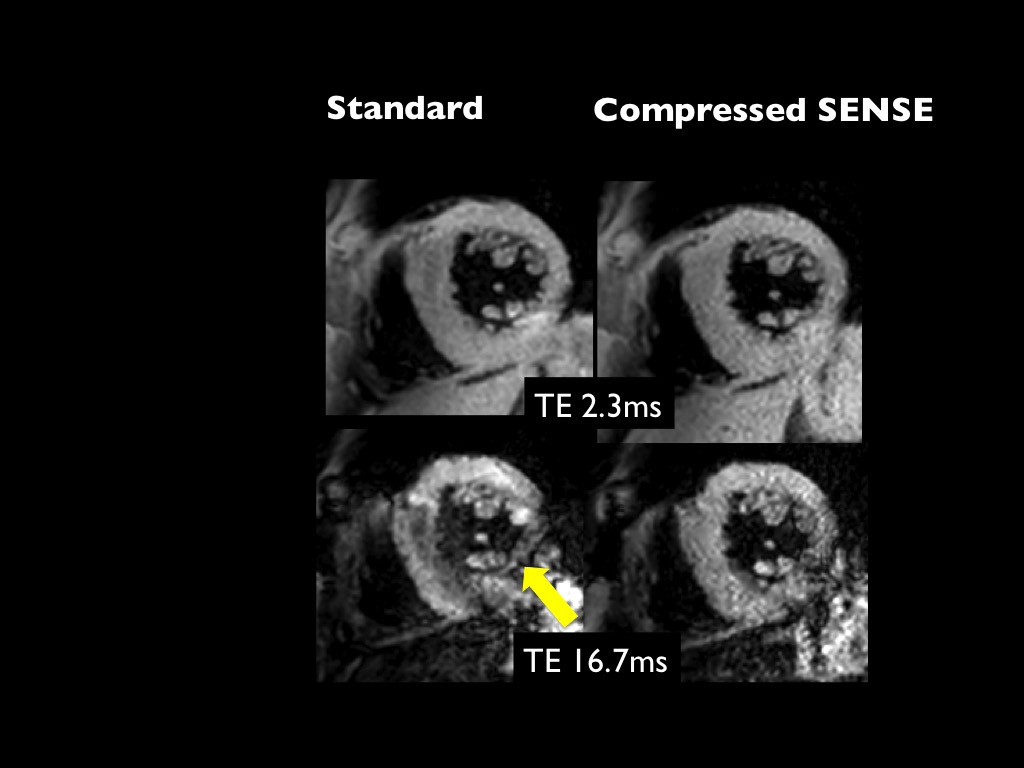
Figure 5. Advantage of Compressed SENSE.
The left side is the standard T2* image and the right side is T2* image with compressed SENSE. Compressed SENSE enables to shorten scan time (20 to 13 sec.). In addition, there is a less motion artifact in the infero-lateral wall on T2* image with an echo time of 16.7msec (arrow, lower row).